Community Partnership Program Grants

The Community Partnership Program aims to reduce the cancer burden statewide
The OHSU Knight Cancer Institute, in its overarching mission to end cancer as we know it, developed the Community Partnership Program in 2014 to reduce the cancer burden statewide. From the beginning, the program has focused on three guiding principles: grantmaking, building communities’ capacity and enhancing community collaboration. Grants fund projects anywhere along the cancer continuum from prevention and early detection to survivorship.
Mission and guiding principles
The mission of the Community Partnership Program is to work hand in hand with Oregon communities as allies in the Knight Cancer Institute's efforts to end cancer as we know it. We aim to:
SUPPORT Oregon communities in identifying and addressing their most pressing cancer-related needs.
FOSTER the skills and abilities of Oregon communities to ensure efforts to address local cancer issues are sustainable long-term.
ENHANCE collaboration between Oregon communities and OHSU to address local cancer issues and cancer health disparities.
The Community Partnership Program has awarded $6.6M to 246 projects
To date, the program has invested $8.8M in 246 projects across Oregon, which includes $6.6M in grant awards. While over two-thirds of the program budget directly funds projects, about one-quarter goes toward funding grantee support that provides trainings on project design and evaluation, carries out program evaluation, and supports costs to bring grantees to an annual conference to share learnings. Approximately 10% of the program budget is directed to administrative costs to support the grant submission platform, distribution of awards, and organizing the annual grantee conference.
Videos highlight projects across the state
To celebrate the program's 10th anniversary, we created videos featuring grantees across the state. Open video playlist on YouTube.
Featured grant recipients: Asian Health & Service Center (Portland), Chelsea's Closet (Tigard), Get Outside After School Activity Program (La Grande), Southern Oregon Friends of Hospice / Celia's House (Medford), and Thadd's Place (John Day).
Grants fund projects from cancer prevention through survivorship
We created the Community Partnership Program to support the development of sustainable collaborations with Oregon communities to address community-identified cancer needs. Grants fund projects anywhere along the cancer continuum from prevention through survivorship. Projects range from the implementation of a community needs assessment about tobacco prevention to supporting the expansion of an existing cancer education program for elementary school students.



Training and technical assistance
Applicants and grantees are offered a range of training and technical assistance resources to support project development, guide projects towards evidence-based practices and assist with evaluation measures.
Addressing cancer-related health disparities
We highly encourage proposals that focus on addressing cancer-related health disparities and increasing equity for Oregon communities that have been historically disadvantaged and/or marginalized.
Applicants are encouraged to submit proposals that use evidence-based approaches to address cancer-related health disparities, including disparities related to race, ethnicity, socioeconomic status, gender identity, sexual orientation, geographic location and disability.
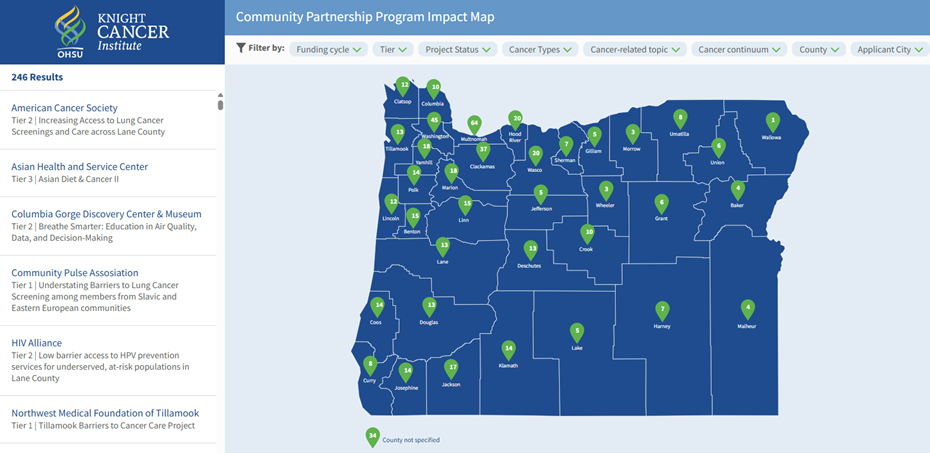
The program has funded projects in all 36 Oregon counties
Completed projects have reached more than 145,000 Oregonians; 38% of projects address cancer issues exclusively in rural communities, while an additional 41% address include both rural and urban communities and 21% focus exclusively on urban communities.
Program Leadership
Co-directors
Questions?
Email us at KnightCancerCRO@ohsu.edu or call 503 418-8077.
Please reach out, we would be happy to speak with you.
Steering Committee
Our steering committee supports the Community Partnership Program by providing strategic direction and making funding recommendations to Knight Cancer Institute leadership.
- Andrea Lara, M.D., M.P.H.: Provider Outreach & Engagement Strategist, Oregon Health Authority
- Jamie Thompson, M.P.H: Senior Research Associate, Kaiser Permanente Center for Health Research
- Jen Olson, M.S., M.A.: Chronic Disease Program Manager, Native American Rehabilitation Association of the Northwest, Inc.
- Kyle Pfaffenbach, Ph.D.: Associate Professor, Eastern Oregon University
- Lisa Parks, B.A., Strategic Initiatives and Training Manager, Willamette Health Council
- Patricia Selinger, M.P.H.: Retired; Breast and Cervical Cancer Program Health Educator and Manager, Oregon Health Authority
- Samantha Watson, M.S.: Director of Community Health Partnerships, Jackson Care Connect
- Taylor Smith, M.B.A.: Disability Services Coordinator, Eastern Oregon University