Oregon Journal Of Orthopaedics | Volume X, 2021
Featured articles from this issue:
- New Faculty Spotlight: Travis Philipp, M.D.
- New Faculty Spotlight: Bopha Chrea, M.D.
- Orthopaedic Adaptations in Undergraduate Medical Education during COVID-19
- Is Less More? Lessons Learned Amidst COVID-19 and the 2021 Orthopaedic Residency Match
- Program Director Kenneth Gundle Uses Instagram to Highlight OHSU’s Strengths During the Pandemic
- Checking in with the Portland Veterans Hospital
- Checking in with Pediatric Orthopaedics at Doernbecher Children’s Hospital
- Checking in with Shriners Hospital for Children
- Checking in with Legacy Emanuel Medical Center: An Interview with Craig Gillis, D.O.
- Checking in with Geriatric Trauma at Providence St. Vincent
- Checking in with Samaritan Health Services: A 2021 Residency Update
- A Research Update at the Portland VA : Striving to Better Define Mechanical Symptoms from Meniscal Pathology
- OHSU’s New Orthopaedic Surgery Alumni Association
- Dr. Robert Orfaly Begins New Leadership Position for AAOS
- Update on the Hayhurst Endowment
- OHSU’s Department of Orthopaedics & Rehabilitation Thanks Dr. Jung Yoo for 15 Years of Service as our Chairman
New Faculty Spotlight: A Q&A session with Travis Philipp, M.D.

By: Ellliot Cole, M.D.
Hometown: Olathe, KS;
Medical School: OHSU;
Residency: OHSU;
Fellowship: NYU;
Favorite Restaurant in Portland? Mediterranean Exploration Company
What’s your go-to OR music? Whatever the resident/fellow I am working with wants
What show(s) are you streaming right now? I recently watched a couple of episodes of Yellowstone
Tell us a little about yourself. I moved to Portland after finishing college at the University of Kansas. Having done both medical school and residency here, I’ve been in the area for about a decade now and love it. I have a wonderful wife, Christian. No kids yet. We take full advantage of living in the PNW by hiking or going to the coast or mountains whenever we have the chance to.
What brought you back to OHSU? We have a great department - I’ve learned a lot from both Dr. Yoo and Dr. Lin and jumped at the chance to be their Jr. Partner. I also like the opportunity to take care of people from all over the state and from all walks of life. Lastly, my wife and I really like Portland.
What made you choose Spine as a specialty? I really like the breadth of the field. In the same day you can do a small MIS discectomy using the microscope and then a large multilevel open procedure. You see patients with degenerative issues, deformity issues, tumors, infections and trauma.
Favorite thing about Portland/PNW? It’s a beautiful area of the country with easy access to the outdoors, mountains and ocean.
What are some goals you have for your practice? The cases that come to OHSU from the community are often complex and offer challenges from both a diagnostic and operative standpoint. I am adding to my operative and diagnostic skills to manage these complicated cases efficiently and effectively. I would like to bring robotic assist technology to OHSU as this technology matures, bringing expanded benefits for patient care.
What are some lessons learned while helping treat COVID patients during your fellowship year in New York? Stay humble. As an orthopaedic spine fellow I certainly didn’t expect that I would spend part of my fellowship year working as a medicine doctor, but 2020 was an odd year. I really had to lean on the more junior medicine residents I was working with. It was inspiring to see how the hospital mobilized to deal with the huge influx of COVID patients.
Do you have any research interests or projects you’re looking forward to pursuing? I would like to get OHSU enrolled and active with the American Spine Registry - a joint registry between the AAOS and AANS. This would add value both from a research standpoint and a quality standpoint. The spine center has already done a lot of great work in terms of rolling out PROs and getting involved with this registry is the next step. I am also interested in exploring the effects of our bundled payments initiative for spine surgery and the effects of being in a bundle vs not. I am currently working on evaluating the effects of a short steroid course after fusion procedures on postoperative outcomes - a project started by Dr. Yoo.
Any advice for the graduating chiefs? Keep working hard as fellows as the jump from fellow to attending is a big one even. Think carefully about how you would manage each patient you see. If your attending makes a different decision, be sure to know why. Keep a print or digital log of your cases that you add to throughout the year. Note the subtle things your attending may do to make the procedure go smoother- things that you won’t be able to find in a textbook etc. Enjoy the year!
New Faculty Spotlight: A Q&A session with Bopha Chrea, M.D.

By: Connor Pihl, M.D.
Hometown: Tillsonburg, Ontario, Canada
Medical School: Trinity College
Residency: University of Mississippi Medical Centre
Fellowship: Foot and Ankle Surgery, Hospital for Special Surgery, New York, NY
Favorite Restaurant in Portland: I wish I knew (Re: COVID)
Go-To OR Music: Hip Hop BBQ
Tell us a little about yourself. I was born in a refugee camp in Thailand, but grew up in a small rural town in Ontario, Canada. My husband grew up in the Pacific Northwest. We have two small children (3 years old and 8 months old).
What brought you to OHSU? I knew early on in my orthopedic training that I wanted to pursue an academic job. Mentors and educators have meant everything to my career and I wanted to work where I could teach and provide the same mentorship to others. On top of that, OHSU also allows me to maintain my involvement in research and continue to push our field into the future. Our extended family is also concentrated in WA and OR so we are very happy to be back home.
What drew you to Foot & Ankle as a subspecialty? I enjoy helping my patients get back on solid footing so they can live, work, and play to their full potential. On top of this, Foot and Ankle encompasses so many of the respective orthopedic subspecialties (arthroplasty, trauma, sports, peds, oncology) that we perform a myriad of different procedures. Foot and Ankle is also still a young field and as such there is a rich spirit of collaboration with my colleagues at OHSU and in the broader community across the world.
What are some goals you have for your practice? My practice goals include a concentrated mix of soft tissue procedures, trauma, and sports. I’d love to continue my involvement in research as well as education both with the medical students and residents. I have a strong desire to make an annual mission trip to provide medical services to underserved patients abroad a part of my practice.
Do you have any research interests or projects which you are looking forward to pursuing? I am in the process of publishing a peroneal tendon reconstruction study, minimally invasive vs open bunion analysis, and weightbearing CT study that was a collaborative effort with surgeons in the US, Brazil, and China. After that, I always have a long list of research questions I hope to pursue.
What has been the greatest challenge in transitioning from fellowship to being an attending? While residency and fellowship prepare you with the surgical tools and medical decision making skills necessary to operate at a high level, only experience teaches you how to shoulder the heavy weight of responsibility that comes with being an attending surgeon.
Favorite things about Portland/PNW so far? I’m loving the trees and beautiful outdoors, great food and drink, and the general attitude of openness and acceptance of others.
Orthopaedic Adaptations in Undergraduate Medical Education during COVID-19
By: David Cornwell, B.S.; Stephanie Zhao, M.S.L.; Zachary Working, M.D.; Lara Atwater, M.D.; Kenneth R. Gundle, M.D.
The COVID-19 pandemic has been an incredible disruption to the American medical education system. During the initial months of the pandemic, medical schools across the nation weighed the decision to allow medical students to continue their hospital training. Questions of adequate spacing, personal protective equipment supplies, and the risk of COVID-19 exposure swirled, especially in the spring of 2020. While medical students were able to return to the wards and operating rooms by the summer, restrictions remained. Two of the most impactful decisions made during this time were the cancellation of in-person residency interviews, and the cancellation of visiting sub-internships. These changes required responses, both for our residency program, and in our support of OHSU students applying for orthopaedic surgery residency.
Orthopaedic surgery residency spots are competitive, with the 2020 NRMP data showing 1,192 applicants for a total of 849 positions, or 1.4 applicants per position. Due to this, students typically complete three to four sub-internships at different institutions. These sub-internships not only prepare students for an orthopaedic residency, but also allow institutions to evaluate applicants on their clinical acumen, work ethic, and attitude. With COVID-19 forcing many hospitals to preserve PPE and limit unnecessary patient interaction, many medical students were not only unable to attend rotations away from their home rotation, they were also unable to practice the requisite skills needed to excel on an orthopaedic sub-internship rotation.
During this time of change, the OHSU Department of Orthopaedics & Rehabilitation took several steps to mitigate the impact of COVID restrictions. The first was to create enough home-institution sub-internships to allow our OHSU fourth-year medical students ample opportunities for rotations without completing travel to other institutions. Rather than one 4-week rotation, we were able to ensure at least 3 months of rotation opportunities. This measure, alongside faculty advising and their hard work, was thankfully successful. There were six aspiring orthopaedists who began their final year of medical school at OHSU during the pandemic; all successfully matched into orthopaedic surgery residencies - more than any other year in the past decade per the publicly available Match lists provided by OHSU School of Medicine.
Another step taken by the Orthopaedics department was to increase their online presence. This effort was multifocal, and included the effective utilization of social media networks such as Instagram and Twitter. The OHSUOrtho Instagram page which highlighted research accomplishments, resident and faculty adventures, and orthopaedic events quickly collected over 1,000 followers in less than 9 months. There is a separate article in this edition about the online expansion, which included efforts to improve the online presence of OJO.
While an immediate focus was the Class of 2021, the OHSU School of Medicine Class of 2022 was also impacted by a multi-month cancellation of clinical rotations. For those in both classes that were interested in exploring orthopaedic surgery in the spring of 2020, a “Remote Introduction to Orthopaedics Surgery” clerkship was created. Multiple faculty came together in a period of less than a month to build an open-ended curriculum guided by overarching objectives to immerse students in the practices of orthopaedics, and prepare them for sub-internships. Many of its objectives were essential to all practices of medicine: familiarity with high impact research and landmark literature, as well as efficient collection and organization of patient data into concise, directed presentations. Other goals, such as interpreting radiographic imaging and classifying fractures, were more specific to orthopaedics. Students were also encouraged to practice suturing and knot tying, fundamental skills that are historically taught in the operating room. Students uploaded their suturing, knot-tying, and fracture descriptions onto an online video sharing platform. Their progress was supervised by faculty surgeons, as well as fellow students, who were able to view each other’s suturing techniques. On a weekly basis, students received fracture radiographs from the course directors, and would practice presenting these fractures orally. These recorded oral presentations were then drawn by fellow students both to give feedback as to the accuracy of the oral presentation and to practice translation of a presentation into a mental image. The actual radiographs were later uploaded so students could compare with their drawings. The Department of Orthopaedics & Rehabilitation allowed students to remotely join in a variety of Departmental lectures, and orthopaedic residents who were present at many of these talks were excited to mentor medical students through difficult concepts as well as the pathway to residency.
The OHSU Class of 2023 was least clinically impacted by the pandemic, but nonetheless had setbacks in their education. One of the hallmarks of the Orthopaedic Surgery Interest Group was monthly research meetings, which took place in person prior to the pandemic. These research meetings were a valuable resource for students with emerging interest in orthopaedic surgery, and allowed them to find research projects and connect with mentors. Thankfully, the new faculty advisor for OSIG, alongside Dr. Natalie Zusman and other residents, were able to successfully transition these meetings online, maintaining the consistency of student research. The ongoing success of OSIG is well shown by at least 30 accepted abstracts from the Department at the 2021 OHSU Research Week, accounting for over 15% of all presentations.
While medical students are thankfully back on rotation, ongoing impacts remain. The 2021-2022 application cycle will have its own challenges and responses. We have learned much in the past year; with flexibility and a determination to continue our educational missions, we will be able to meet what follows.
Is Less More? Lessons Learned Amidst COVID-19 and the 2021 Orthopaedic Residency Match
By: Henry M. Fox, M.D.; Kenneth R. Gundle, M.D.
Framing the issue
The famous mathematician John Von Neumann, in his 1928 “minimax theory,” established the concept of zero-sum games—in which each participant’s gain or loss of utility is precisely balanced by the utility gains or losses of other participants.1,2 Several of Von Neumann’s tenets can be applied to the high-stakes orthopaedic surgery match. Two key stages of the Match process, the Roth-Peranson algorithm,3 are conceivably “zero-sum”: interview positions, and residency positions. Applicants vie for a finite number of positions, and the benefit to one applicant (occupying a spot) is directly proportional to the loss of another (being unable to occupy said spot).
In order for an applicant to attain residency positions, interview invitations must be obtained. The competition amongst applicants for invitations is decidedly not zerosum: the relative value of an interview invitation for applicant A is likely disproportional to the relative value of that same invitation for applicant B. Applicant A may have a small gain of utility from this invitation, if he or she already has fifteen invitations. Applicant B may have a large gain of utility from the invitation, if he or she has a fewer-than-desired number of invitations. This is reinforced by the National Residency Matching Program (NRMP) “Charting Outcomes in the Match.”4 Above 14-15 ranked programs, an applicant’s probability of matching only incrementally increases with each additional interview, whereas for applicants with fewer interviews, each additional interview can drastically increase the probability of matching. Herein we propose an alternative strategy for applicants to obtain a satisfactory number of interview invitations, in a manner that is simultaneously conscientious of programs.
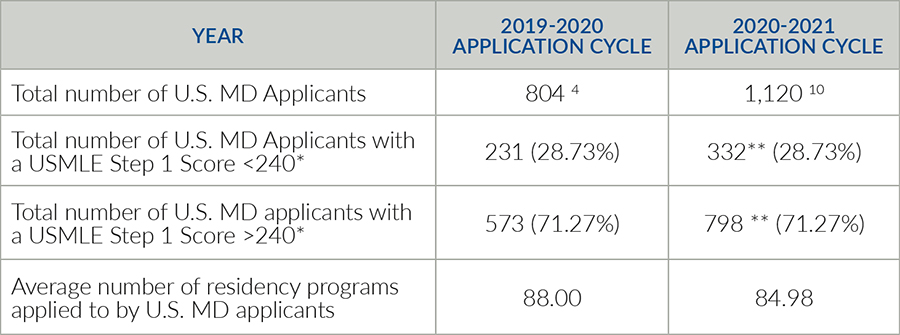
Table 1. USMLE: United States Medical Licensing Exam. * Note that due to limitations in data granularity (i.e., distributions of Step 1 exam scores reported in increments of 10) we could not choose the precise AOA/CORD Recommendations cutoff of a 235 Step 1 score. Instead, we chose a higher cutoff of 240. ** Note that for the 2020-2021 cycle, the total number of applicants with a given exam score is extrapolated from the distributions of exam scores from the 2019-2020 cycle. We assumed that this distribution remained comparable across these two years. With the average number of programs applied to and the number of 2020-2021 applicants, the total number of orthopaedic applications is 95,177.6.10 Assume that each applicant with a Step 1 score >240 applied to 40 programs. 95,177.6=x(322)+40(798), where x equals the number of programs that applicants with a Step 1 score 240 applied to 40 schools, then the average applicant with a Step 1 Score <240 would have had to apply to 196.45 training programs. There were 190 participating programs in 2021.
Changes (and Sequelae) in the 2020-2021 Orthopaedic Application Cycle
In response to this year’s sweeping changes to the application cycle,5 in May of 2020 the American Orthopaedic Association’s Council of Orthopaedic Residency Directors (CORD) urged allopathic applicants with United States Medical Licensing Exam (USMLE) Step 1 scores greater than 235 to apply to fewer than forty programs.6 If a decreased volume of applications per program were to occur, then applicants would theoretically benefit from a more holistic review of their application.7–9
It appears that the CORD recommendations were not widely heeded (Table 1). Preliminary 2021 ERAS data demonstrates that the average number of orthopaedic programs applied to—for U.S. allopathic students—was 84.98, down from 88.00 in 2020.10 While this is a downturn in the average number of applications trendline7 the average number of applications per program increased, from 590.27 applications in 2020 to 619.59 in 2021.10 This increase is not attributable to the combined DO and MD match. While further data is surely forthcoming, the collective decision of applicants to widely apply will have harmful sequalae. The American Association of Medical Colleges (AAMC) announced in December 2020 that a maldistribution of interview invitations had occurred.11
Perspectives of an Applicant and a Program Director
From an applicant perspective, the inequity of interview invitations can be countered by proactively getting to know programs that one is truly interested in—and limiting applications to these programs alone. One author (HMF) applied to 39 orthopaedic residency programs during the 2020-2021 cycle. He had average USMLE Step 1 and Step 2 Clinical Knowledge (CK) scores for matched orthopaedic applicants, strong clinical grades, and a relatively strong research background; he was selected into the Gold Humanism Honor Society (GHHS) but not Alpha Omega Alpha (AOA). He wrote a programspecific paragraph in each personal statement. His application also included, “I have followed the AOA/CORD recommendations and submitted applications to no more than 40 programs.” He declined several interviews and interviewed at twelve institutions; in nine interviews either the chairperson, program director, or associate program director specifically commented on his adherence to the AOA/CORD guidelines.
Prior analyses have attempted to calculate the number of applications required to obtain twelve interviews, based on applicant features like AOA membership and board exam scores.12 However, these analyses are unable to account for the critical importance of a) students interfacing with programs prior to applying, b) writing genuine, thoughtful program-specific paragraphs in personal statements, and c) signaling that the applicant is only applying to programs he or she is truly interested in. This can be done in concert with away rotations, which will hopefully resume in August of 2021.13
From a program director’s perspective (KRG) there is value in knowing the number of programs that an applicant is applying to. In concert with other factors, it allows one to gauge an applicant’s degree of interest. In typical years, away rotations are the gold standard of an applicant indicating interest. Away rotations are educational, and an opportunity for programs and applicants to get to know each other on the ground. These rotations are ascribed significant weight in the applicant evaluation process and have been shown to correlate with Match success.14–16 Yet the number of away rotators is relatively limited in comparison to the total number of distributed interview invitations. To fill this program interest void between away rotators and the remaining applicant pool, knowledge of the number of submitted applications could help program directors further evaluate and gradate the interest of applicants.
Future Considerations and Actions for Stakeholders
While individual decisions must be made by each future applicant, we urge applicants and their mentors to consider a more targeted approach in future application cycles. There is little correlation between an orthopaedic applicant’s qualifications and the number of programs applied to17; strong applicants should feel empowered to adopt a more deliberate tactic. We also suggest that applicants (and/or Letter of Recommendation writers) consider reporting the number of programs to which an applicant has applied.
In future years, we urge the AAMC’s Electronic Residency Application Service (ERAS) to report the number of programs applied to by each applicant. The addition of this pressure—which would encourage more targeted applications—will become increasingly important as the USMLE Step 1 exam transitions to Pass/Fail grading, and programs strive for a more holistic application review of applicants.8,18–20 Hopefully we could avoid the added work, for applicants and programs alike, of secondary essay requirements.7 Currently there are simply too few mechanisms that encourage or reward applicants who thoughtfully select a smaller number of programs of interest. If one believes in the holistic review of applications, then he or she should support such efforts to change the procedural landscape.
Orthopaedic surgery is perennially one of medicine’s most competitive specialties.4 Unless action is taken, a yearly deluge of applications upon programs—and an inequitable distribution of interview invitations for applicants—will likely persist. These consequences harm residency programs and applicants alike. The orthopaedics community must leverage its position to explore, alongside other stakeholders such as the NRMP and ERAS, how to best refine the application process. We hope that in the future, the alignment of interests will facilitate an improved orthopaedic Match process for all.
References
- von Neumann J. Zur Theorie der Gesellschaftsspiele. Math Ann. 1928;100:295-320.
- Kjeldsen TH. John von Neumann’s Conception of the Minimax Theorem: A Journey Through Different Mathematical Contexts. Arch Hist Exact Sci. 2001;56(1):39-68.
- Maaz M. A Primer on the Game Theory Behind the National Resident Matching Program for the Medical Educator and Student. Med Sci Educ. 2020;30(2):965-969.
- Charting Outcomes in the Match: Senior Students of U.S. MD Medical Schools. Characteristics of U.S. MD Seniors Who Matched to Their Preferred Specialty in the 2020 Main Residency Match. Published online July 2020. Accessed January 25, 2021.
- Aiyer AA, Granger CJ, McCormick KL, et al. The Impact of COVID-19 on the Orthopaedic Surgery Residency Application Process. J Am Acad Orthop Surg. 2020;Publish Ahead of Print. Accessed March 1, 2021. https://journals.lww.com/10.5435/JAAOS-D-20-00557
- AOA Council of Orthopaedic Residency Directors (CORD). Letter to Orthopaedic Surgery Residency Programs. Published online May 27, 2020. Accessed January 25, 2021. aamc-orange.global.ssl.fastly.net/production/media/ filer_public/74/44/7444d6bc-5148-49b0-b240-cf90130b943a/ aoacord_rec_guidelines_2021_application_seasonaamc.pdf
- Trikha R, Keswani A, Ishmael CR, Greig D, Kelley BV, Bernthal NM. Current Trends in Orthopaedic Surgery Residency Applications and Match Rates. J Bone Jt Surg Am. 2020;102(6):7.
- Bernstein J. Not the Last Word: Ending The Residency Application Arms Race—Starting with the USMLE. Clin Orthop. 2016;474(12):6.
- Bernstein J. Not the Last Word: Roll Them Bones—Selecting Orthopaedic Surgery Residents by Lottery. Clin Orthop. 2019;474(12):2535-2638.
- Electronic Residency Application System. Preliminary Residency Application Data (ERAS 2021). Published online January 13, 2021. Accessed January 25, 2021. https://www.aamc.org/data-reports/interactive-data/eras-statistics-data
- Whelan A. AAMC Open Letter on Residency Interviews from Alison Whelan. Published online December 18, 2020.
- Chen AF, Secrist ES, Scannell BP, Patt JC. Matching in Orthopaedic Surgery: J Am Acad Orthop Surg. 2020;28(4):135-144.
- The Coalition for Physician Accountability. Medical Student Away Rotations for Remainder of 2020-2021 and 2021-22 Academic Year. American Association of Medical Colleges; 2021. Accessed January 25, 2021.
- Camp CL, Sousa PL, Hanssen AD, et al. The Cost of Getting Into Orthopedic Residency: Analysis of Applicant Demographics, Expenditures, and the Value of Away Rotations. J Surg Educ. 2016;73(5):886-891.
- Baldwin K, Weidner Z, Ahn J, Mehta S. Are Away Rotations Critical for a Successful Match in Orthopaedic Surgery? Clin Orthop Relat Res. 2009;467(12):3340-3345.
- Porter SE, Jobin CM, Lynch TS, Levine WN. Survival Guide for the Orthopaedic Surgery Match. J Am Acad Orthop Surg. 2017;25(6):403-410.
- Finkler ES, Fogel HA, Kroin E, et al. Factors influencing the number of applications submitted per applicant to orthopedic residency programs. Med Educ Online. 2016;21(1):31865.
- Salari S, Deng F. A Stepping Stone Toward Necessary Change: How the New USMLE Step 1 Scoring System Could Affect the Residency Application Process. Acad Med. 2020;95(9):1312-1314.
- Lin GL, Nwora C, Warton L. Pass/Fail Score Reporting for USMLE Step 1: An Opportunity to Redefine the Transition to Residency Together. Acad Med. 2020;95(9):1308-1311.
- Moynahan KF. The Current Use of United States Medical Licensing Examination Step 1 Scores: Holistic Admissions and Student Well-Being Are in the Balance. Acad Med. 2018;93(7):3.
Program Director Kenneth Gundle Uses Instagram to Highlight OHSU’s Strengths During the Pandemic
By: Kenneth Gundle, M.D.
Our people are such a strength of the residency and the Department. Each individual’s attributes are then compounded by the collegial way we interact on a daily basis - finding humor, support, sibling-like rivalries and moments of joy.
Yet as words and statements, these truths and our positive idiosyncratic culture may seem all-too replicable; people manage to say and write all sort of things these days. Experiencing on-the-ground lived reality for a few weeks is a far superior way to know these things themselves.
This is not a complicated argument to make, especially to orthopaedic surgeons or those who aim to join the field. If someone is talking about a complicated operation that went really well, then we’d sure like to see the x-rays. This mindset undoubtedly contributes to medical students traveling all over the country for ‘away rotations’ - subinternships with orthopaedic surgery programs of interest. And in addition to the educational value, all parties gain from spending time together and seeing if joining forces for another 5 years seems like a good idea.
For the class graduating in 2021, these away rotations were not really an option. COVID-19 restrictions prevented any medical students from conducting away rotations at OHSU. Our only advantage in this suboptimal scenario was in seeing it coming. So how to respond? How can we share of ourselves in a way that celebrates what we are, while also making possible for interested external groups of people to see us in a more authentic way?
These questions were the driving forces in joining Instagram. Sharing pictures is not as much fun as an afternoon SAFETY Meeting at F&B. But it could be a way to stay connected with each other, while reflecting our days and our ways. That was its inner-directed objective. Additionally, these pictures could be a window for medical students applying in orthopaedic surgery to see our program in a way that a website or a virtual interview struggle to convey. What do we celebrate? How seriously do we take ourselves? What is it with OR shoes and socks in this program? Do all the residents have (and obsess over) pets? And while nothing can match the in-person beauty of a summer sunrise over Mt. Hood from the Tram, we can post dozens of pictures and videos to give it a go. Pictures of trail hikes, snowboarding, garden successes, bike rides and big catches project what we are up to and things we value. Pictures of call teams, Arthroscopy Boot Camp, awards and the Wall of Research show what we are up to while on the Hill. And of course, Dr. Doung’s pipe cleaner animals are absolute works of art for which she clearly needs a social media savvy agent who receives a modest 60% of proceeds… just saying.
With Instagram, we can share a bit of ourselves. My hope is that it served a role of keeping us together while too-often apart this past year. I also think our posts were a great reflection of our Program and values, to anyone who may have taken a look. And as it continues, I think it’ll serve helpful in keeping our graduates engaged and interested in the Department for years to come. So slam that follow button, and throw us a few ‘likes’ TW: @OHSUOrtho | Insta: ohsuortho
And since the IG is all about them pics… here are some highlights from the past year!

Checking in with the Portland Veterans Hospital

By: David Cornwell, B.S.
There is not a medical institution in the country, likely not a household in the country, which has not experienced change in this past year. The Portland VA orthopaedics group was by no means exempt from the wave of change that swept the country. As COVID-19 spread, it drove change in the existing systems architecture, highlighting strengths and areas for change.
At the Portland VA, non-emergency surgeries were severely curtailed last spring. To help PPE supplies, a complex system of UV sterilization was instituted by members of the anesthesiology group – this helped keep N95 masks available throughout the duration. To help minimize in-person visits, virtual clinics were expanded through the already present VA Video Connect (VVC) system. This built on a system of eConsults and remote care that had already been in use by Dr. Gundle for tumor referrals, among others. A benefit of familiarity with VVCs going forward is a decrease in unnecessary travel for rural patients (including from Idaho!), as well as those who are recovering at the VA Community Living Center in Vancouver and Roseburg.
Slowly, the VA has been able to bring back elective surgery. Outpatient operations, especially arthroscopic procedures with Dr. Berkson, were able to return faster and keep education going. Surgical volumes are now recovering, which is great for residents, faculty, and most of all our patients. And we must mention the great response of the Portland VA in administering vaccinations rapidly. This was done in part by volunteers from the orthopaedics section working in vaccination clinics. The team was also able to see a patient in clinic, then send them the same day for their first shot – and now some members of their family as well! The Portland VA orthopaedics group looks forward to the upcoming year, and improving as a close-knit team.
Checking in with Pediatric Orthopaedics at Doernbecher Children’s Hospital

By: Scott Yang, M.D.
The Pediatric Orthopaedics service at OHSU has been providing excellent care for children and adolescents throughout the Pacific Northwest. 2020 was an interesting year, both in adjusting to, and providing care during the COVID-19 pandemic. Our service has not stopped despite the lock downs, as we found that earlier in the pandemic we were even busier with children getting hurt as they were all out of school!
From a clinical care perspective, we aim to provide an intersection of current / cutting edge clinical care, and the best patient outcomes. In 2020-2021, we have remained busy from a trauma perspective (treating femur fractures, elbow fractures, etc.), and have provided complex care such as magnetic femoral or tibial lengthening procedures, limb deformity corrections, scoliosis corrections, and complex surgeries in children with neuromuscular conditions. For some complex congenital scoliosis conditions, sometimes the anatomy is very atypical, and we have been utilizing 3D printing to create a 1:1 ratio model of the spine before performing surgery - to study, and also practice, prior to performing the operation. By the time the child is on the operating room table, we have already understood the spine completely by studying and manipulating the model. We have also been collaborating with the main hospital at OHSU to utilize CT navigation for complex spine surgery to provide as perfect as possible placement of spinal hardware for challenging spine cases. Our goal has been, and will continue to be to intersect technology, outcomes, to provide quality care with maximal patient safety.
We all love what we do, and try to provide the best educational experience for our trainees as well. We have been active in the research front with several publications and national presentations to put us on the map. We are active in several multicenter studies, and have been contributing to an international research group in Perthes Disease. We are also proud to be amongst the top in the country, as we are distinctly ranked in the top 50 pediatric orthopaedic services in the United States based on US News and World Report. From a personal perspective, all the providers on the pediatric orthopaedics team have been trying to maintain a balance with life and work. If you live in the Portland area, you will likely see Dr. Matthew Halsey running along Terwilliger Blvd, Pollee Brookings NP running some ridiculous >50 mile trail races, and Dr. Scott Yang cycling the west hills of Portland.
Checking in with Shriners Hospital for Children

By: Jeremy Bauer, M.D.
Like many programs the biggest change to our education has been virtual conferences. This has led to some opportunities; we have been able to increase the accessibility of our quarterly Grand Rounds to not only those able to make it here in person, but also to any interested participant. It has also made it easier to have speakers that would not have been able to attend because of the same geographic restraints.
Our department has seen the retirement of two beloved surgeons, Michael Aiona, M.D., and Michael Sussman, M.D. Both surgeons have served as Chief of Staff at the Portland hospital, and have an incredible legacy of education, research, and excellent patient care. Luckily, they have both agreed to become emeritus professors and have already stayed engaged in our Wednesday morning educational series as well as our weekly Motion Analysis Center meetings.
Thanks to the approval and support of the OHSU Orthopaedic and Rehabilitation Department and the OHSU office of Graduate Medical Education, senior OHSU orthopaedic residents have been taking call at the Shriners Hospital. This has led to excellent coverage of our inpatient ward and has allowed the PGY-2 residents more clinical time. Our partnership with OHSU is expanding to our Motional Analysis Center (MAC), allowing children with gait abnormalities at OHSU to be seen and evaluated in our MAC.
Checking in with Legacy Emanuel Medical Center An Interview with Craig Gillis, D.O.

By: David Cornwell, B.S.
What a year it has been. 2020 will forever hold a place in the books of our generation. I think we all remember the harsh transition beginning in March of 2020, when everything changed and the country shut down. Elective surgeries were halted across all hospital systems and no one knew what the future held for managing this new virus. Unfortunately, a moratorium on elective cases does not stop traumas from happening. Being one of only three level 1 trauma centers in the Pacific Northwest, Legacy Emanuel manages a significant amount of orthopaedic trauma and thus our surgical cases are oftentimes urgent or emergent. In the face of this pandemic, navigating orthopaedic trauma proved difficult.
While the medical community diligently worked to address COVID-19, logistical barriers continued to plague most healthcare systems - including access to N95s and PAPRs. One of the biggest initial hurdles we encountered was managing trauma patients with limited COVID testing. We had days where the entire hospital had less than 5 rapid tests available. This meant any traumas beyond that volume were presumed COVID positive until proven negative. A number of cases were treated as such, meaning our surgical team was lucky enough to wear an N95 throughout some grueling cases. Despite these initial challenges, Emanuel was able to appropriately address most of these issues and maintain a reserve of testing and PPE to ensure our trauma patients received exceptional care.
As we settle back into a rhythm in balancing our trauma and elective cases, Summit Orthopaedics and Emanuel have developed an excellent system to ensure all patients are managed in a timely manner. Preoperative COVID testing continues to be required for every case but has become easy and reliable for patients to obtain. From an elective standpoint, our arthroplasty service is growing and we are expanding our utilization of patient specific instrumentation including in shoulder arthroplasty. Drs Madey, Frome, and Gillis continue with coverage on all upper extremity cases and microvascular procedures. The lower extremity service with Drs Mirza and Vande Zandschulp also remains extremely busy, and is likely to become even busier as we move into spring and summer.
With a return to a pseudo-normal life, we remain thankful for all of our healthcare workers at Emanuel. Despite the uncertainty COVID initially brought upon us, our team was able to navigate these challenges and remained committed to ensuring patients were cared for. Who knows what the rest of 2021 has in store for us, but we remain hopeful and optimistic in our ability to overcome unforeseen challenges.
Checking in with Geriatric Trauma at Providence St. Vincent

By: Richard Southgate, M.D.
The coronavirus pandemic changed many aspects of the residency education process, from away rotations and the match to the annual in-training exam and clinical rotations.
In March 2020, all elective cases were cancelled in Oregon. This suddenly altered the training experience for resident rotations as hospitals across the state paused all non-emergent cases, including most orthopedic surgeries. Prior to the pandemic, the residents who rotated through Providence St. Vincent had a rotation that mostly exposed them to arthroplasty and sports, with only one day per week covering community trauma. Due to logistical restrictions associated with contact tracing, the ambulatory clinic aspect of the rotation at Providence St. Vincent was removed for residents, practically overnight.
These changes provided us, like many others, an impulse to adapt. We shifted to a purely surgical rotation on the fracture block focused on general and community trauma cases. This gave the residents increased exposure to geriatric trauma, as most cases that come through the emergency department and transfer center at St. Vincent are low energy hip fractures and periprosthetic trauma.
This change for the group at St. Vincent was a sign of how adjustments occurred quickly in the wake of the virus, even within established practices and institutions. When at St. Vincent, OHSU residents work predominantly with surgeons from Orthopedic + Fracture Specialists, a private practice consisting of 16 orthopaedic surgeons who have fellowship training in nine different subspecialties. This group has practiced exclusively at St. Vincent since the group’s founding in 1934. Providence St. Vincent is a 523-bed community hospital—the largest Providence Health & Services hospital in the state of Oregon. The fracture block itself was established over a decade ago by Dr. Darin Friess at OHSU and Hans Moller at Orthopedic + Fracture Specialists. This year, a novel disease brought novel challenges, and even these large, well-established groups and traditions were forced to be nimble to continue providing residents with a well-rounded surgical education and patients with excellent care.
Our new approach worked. Over the last twelve months, 658 cases were completed in the fracture block and on weekends, exposing residents to a balanced mix of community trauma. 68 cases were completed in the fracture block in March 2021. These included 31 geriatric hip fractures (19 hemiarthroplasties and total hips for fracture, 11 cephalomedullary nails, and 1 sliding hip screw), 6 ankle fractures, 6 upper extremity fractures, 6 revision arthroplasties (both elective and for infectious etiologies), 5 irrigation and debridements, 4 periprosthetic fractures, 3 elective arthroplasty cases, 2 closed reductions, 2 tibial nails, and 1 each of the following: pediatric trauma, patella ORIF, and removal of hardware. The residents rotated on trauma cases with Drs. Kimberly Workman, Amer Mirza, Richard Southgate, Jeana Summers, Hannah Aultman, Alex DeHaan, and Mark Manoso. In addition to the orthopaedic surgeons who operate on these patients, there are three full time clinical employees involved in the day-to-day workings of the fracture service plus additional administrators at Providence St. Vincent.
The backbone of our fracture block is made up of our experienced nurse practitioners, Nori Trevarthen and Melissa Thomas. They assist with consults, manage all of the floor work, and are indispensable in caring for our geriatric trauma population. Because we have NPs to assist with patient care duties, the residents are encouraged to focus on preoperative planning for their surgical cases, achieving full independence on certain quotidian community trauma cases by the end of their rotation. The repetition from seeing these hip fractures helps reinforce any pearls that they pick up throughout the rotation. We believe that this helps compliment the higher acuity Level 1 polytrauma they are exposed to at OHSU and Legacy Emanuel. Additionally, it gives the residents a glimpse of what orthopaedic trauma call is like in a community setting, which is unlike a busy urban or academic trauma center.
Although there is an increase in the representation of geriatric trauma on the rotation, there has been a return to some normalcy. The residents still have two days a week with Dr. Duwelius (elective total joints) and Dr. Andres (sports, shoulder replacements, and arthroscopy). This helps round out their experience.
The success of the rotation’s uninvited change in 2020 has given us confidence to continue improving the experience at St. Vincent for residents, patients, and attending surgeons. We have discussed resident involvement in our geriatric hip fracture registry, which would be a first in the Providence health system, and would help expose residents to clinical research opportunities outside of an academic center. Additionally, we hope to grow mentoring opportunities as residents move through the fellowship application process, and we plan to continue involving them in arthroplasty research, as some have done with Dr. Duwelius in the past. We at O+FS and Providence St. Vincent look forward to continuing the collaboration with OHSU’s orthopaedic surgery residency program.
Checking in with Samaritan Health Services: A 2021 Residency Update

By: Teigen Goodeill, D.O.
Like the rest of Oregon, United States, and world, the Willamette Valley was not immune to the Coronavirus Pandemic. Though many were quarantined for long periods of time, patients continued to require musculoskeletal intervention. This led to a truly galvanizing opportunity for our orthopaedic teams as shifts, call schedules, and responsibilities were reshaped in the wake of the pandemic; the program stepped up to the challenge and continued to provide high-quality patient-centric care throughout the Willamette Valley.
The summer and fall seasons typically provide a time where medical students from across the nation interested in the orthopaedic field rotate through our tertiary medical center. This allows students an opportunity to learn the basics of orthopaedic diagnosis, treatment, and patient care. When this educational offering for medical students was put on halt secondary to the pandemic, residents at Good Samaritan Regional Medical Center stepped up to this challenge and produced a virtual lecture series to effectively fill this void. A wide range of topics was presented such as basics of fracture reading, pediatric fractures, and adult hip and upper extremity fractures. Lectures were attended by residents as close as our local medical school in Lebanon, OR to as far away as Brazil. Although we are anxious to see what the future holds in regards to inperson education, our virtual lecture series was so successful and highly attended that we will continue the series in the spring.
The involvement in research-related activities has never been more robust than it is now. Our residents continue to produce meaningful research in multiple subspecialities of orthopaedic surgery. To name a few, Drs. Justin Than and Babe Westlake’s research was accepted for publication in Arthroplasty Today as they evaluated different forms of pain control in total joint arthroplasty. Additionally, we continue to have a great relationship with Randall Children’s Hospital in Portland, OR for our pediatric education which has allowed for multiple publications and research projects to come to fruition. Dr. Shaun Conley was recently published in the JBJS Case Connector as they discussed a case series of spontaneously reduced pediatric incarcerated medial epicondyle fractures while Drs. Justin Brohard and Alexandra Scoles received the Legacy Foundation Grant having instituted a randomized clinical trial which is now in active recruitment regarding pediatric elbow fractures.
A Research Update at the Portland VA Striving to Better Define Mechanical Symptoms from Meniscal Pathology
By: Mark Berkson, M.D.; Samuel Moulton, M.D.; Jorge Walker, M.S.
How did we get here?
In 1940 McMurray delivered a lecture at the Royal College of Surgeons of England describing his method of “manipulation of the injured joint” to identify tears of the “semilunar cartilage” of the knee.1 In 1946, Apley described the “three disadvantages in this method,” and then proposed his test as a better solution for the problem of identifying meniscal tears.2 Their goal was the same, identify the tear, cut out the meniscus, and help the patient. They both had a fair amount of success with the first two goals, but we now know that completely cutting out the meniscus was a bad idea.
Fast forward almost a century and we have MRIs to accurately identify the meniscal tear. We have advanced minimally invasive techniques to remove only the torn fragment. We are still left with a question on the third goal, are we helping the patient?
Where do we need to go?
We face an uphill battle in the public eye and the medical community, to prove we can reliably identify symptoms from a torn meniscus that fail nonoperative treatment and improve with surgery. Randomized trials and editorials have concluded that arthroscopic partial meniscectomy provides no benefit over nonoperative treatment or placebo surgery.3-6 However, studies failed to stratify patients with mechanical symptoms. If equal numbers of patients with mechanical symptoms were randomized to each study arm, it is not surprising that no difference was found between the operative and non-operative arms of the study.
One consensus article across three continents concluded “Once surgical treatment is considered, the burden lies on the surgeon to ensure that the patient’s pain is truly emanating from the meniscal pathology, which at certain times can be difficult if not impossible.”7 We agree and search for a more universally accepted indication for arthroscopic partial meniscectomy.
How do we get there?
Step 1. Establish a universally accepted definition of mechanical symptoms based on history and physical exam findings.
Step 2. Conduct rigorous prospective studies comparing patients with meniscal tears with identified mechanical symptoms against those without mechanical symptoms.
Our retrospective pilot study addressed step 1. We designed a simple, reproducible, binary physical exam test, the Portland Pivot Kick (PPK), to identify symptomatic medial meniscus tears with mechanical symptoms. At an average follow up of 9.8 months (range 1 – 18.7 months), 50 of 51 (98%) patients had a negative PPK test. All 51 patients had a positive PPK test prior to surgery. All KOOS and WOMAC subjective patient outcomes scores significantly improved, by 37% to 53% (P<0.001).
An ongoing prospective study is underway comparing patients with mechanical symptoms who undergo a partial meniscectomy to those who continue nonoperative treatment, to assess the PPK as an objective assessment of mechanical symptoms. We aim to help further define mechanical symptoms and define the subgroup of patients who could benefit from surgery.
- McMurray T. The semilunar cartilages. Br J Surg 1942;29(116):407-14.
- Apley AG. The diagnosis of meniscus injuries; some new clinical methods. J Bone Joint Surg Am. 1947 Jan;29(1):78-84.
- Roos EM, Thorlund JB. It is time to stop meniscectomy. Br J Sports Med 2017;51:490–1.
- Sihvonen R, Paavola M, Malmivaara A, et al. Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013 Dec 26;369(26):2515-24.
- Sihvonen R, Englund M, Turkiewicz A, et al. Mechanical symptoms as an indication for knee arthroscopy in patients with degenerative meniscus tear: a prospective cohort study. Osteoarthritis Cartilage 2016;24:1367–75.
- Sihvonen R, Paavola M, Malmivaara A, et al. FIDELITY(Finnish Degenerative Meniscal Lesion Study) Investigators. Arthroscopic partial meniscectomy versus placebo surgery for a degenerative meniscus tear: a 2-year follow-up of the randomised controlled trial. Ann Rheum Dis. 2018 Feb;77(2):188-95.
- Stone JA, Salzler MJ, Parker DA, et al. Degenerative meniscus tears – assimilation of evidence and consensus statements across three continents: state of the art. Joint Disord Orthop Sports Med 2017;2:108-19.
OHSU’s New Orthopaedic Surgery Alumni Association

By: Elizabeth Lieberman, M.D.
We are excited to announce the formation of an OHSU Orthopaedic Surgery Alumni Association. The aim is to create a network of graduates from the OHSU Orthopaedic Surgery residency program that will serve to connect graduates, honor alumni achievements, and support the residency program. We hope to engage alumni in supporting education, research, and career development for the next generation of surgeons.
A newly formed committee chaired by 2019 graduate Elizabeth Lieberman, MD has begun work planning activities and events to connect alumni locally and at national meetings. Regular communications will provide updates from faculty and alumni to help us stay connected. We are also working on establishing awards and scholarships to support resident and medical student experiences.
All OHSU orthopaedic surgery residency and fellowship graduates will be eligible to join. Stay tuned for more details about membership and upcoming events. Please let us know if you have ideas or suggestions for the association. We look forward to hearing from you! Contact Elizabeth Lieberman at lieberme@ohsu.edu for more information.
Dr. Robert Orfaly Begins New Leadership Position for AAOS

By: Robert Orfaly, M.D.
The world is changing at an ever-increasing pace. No secret there. While scientific discovery and therapeutic innovation lead to the evolution of the care we provide as orthopaedic surgeons, change in how healthcare is delivered is more rapid and less predictable. It, therefore, stands to reason that each of us must take on roles of transformational leadership if we are to keep up with this continuous change and aspire to become true innovators. One of the fundamental aspects of effective change management is communicating well with the entire team. Only in this way can a leader gain the advantage of the rich diversity of knowledge and experiences that a team brings to the table and create a shared vision to benefit the organization.
I always appreciated these truths and sought out leadership roles that fit this model. When choosing a committee assignment within the American Academy of Orthopaedic Surgeons at the end of my Leadership Fellows Program (LFP), I selected the Communications Cabinet. My next role was as a member, and then chair, of the Membership and Leadership Development Committee that focused on member needs and managed the LFP program. I later had the great fortune to be elected chair of the Board of Councilors, which serves grassroots advocacy and communication between the membership and leaders of the Academy. These experiences were put to good use during my term on the AAOS Board of Directors as we redefined our mission, vision, and strategic goals for the next decade. Energized by this experience working with many of the great innovators and leaders in orthopaedic surgery, I was delighted to receive a call from AAOS president Joe Bosco offering me the role of AAOS Now editor-in-chief. As the primary AAOS membership publication, I view this as a critical vehicle for communicating the change necessary for our association and our profession.
In a Harvard Business Review article by Angela Fisher Ricks, the author outlines four steps to communicating organizational change:
- Share a vision
- Tell a story
- Make those in your organization the heroes
- Chart the path.
Whether clinical, advocacy, practice management, or diversity content, every AAOS Now article helps articulate the vision of orthopaedic surgeons as the trusted leaders in advancing musculoskeletal health. This vision is illustrated through education, commentary, and stories about AAOS members who are making a difference. AAOS Now is also an open newsroom in which every single member (yes, you!) can submit an article about your discoveries and experiences. In this way, the publication can serve multidirectional communication as knowledge is exchanged and a path to our common vision is created.
Most recently, I was selected to be one of 20 mentors to the inaugural class of the Level 3 training for the AAOS Leadership Institute. Mentees are competitively chosen for their aspiration and potential for higher levels of Academy service, such as committee or council chair or member of the Board of Directors. As I come full circle in my relationship with the AAOS, I am confident that the efforts of every member can create a shared future of excellence for our patients.
Update on the Hayhurst Endowment

By: Jacqueline Brady, M.D.
The Hayhurst endowment has been an incredible boost in the area of resident education research. The first big move we made was to upgrade the sensors that record motion patterns during arthroscopy. Version 1 of the sensors was a brilliant set of equipment, but required a lengthy and onerous intermediate step using Matlab to process the firestorm of data points obtained during a recording session before true data analysis for research purposes could even begin. With the assistance of the Hayhurst fund, we obtained a set of Version 2 sensors, which skip that step by processing that data themselves into averages that can be analyzed to determine significance as we ask questions of the data. Collection is ongoing as residents rotate through the sports service and participate in simulation labs with practice in the shoulder, knee, and hip. We hope to gather the new data soon to help us understand how arthroscopy of the shoulder and hip joints might inherently differ from the knee, which will direct our educational interventions as residents pick up these new skills.
Meanwhile, we are embarking on another project with funding from the Hayhurst endowment: a study of the “work” of residency using a wearable device to track biometric data. The ACGME requires residency and fellowship program directors to educate trainees about fatigue as they work hard during their residency experiences, but specific information surrounding the effects of various portions of residency is lacking. Michelle Lawson, one of the rising PGY-3 residents, is seeking to understand various questions about sleep disturbance in particular as it pertains to fatigue during residency. A demo group of residents and faculty has been testing the device for the last several months, gathering some tips and additional ideas for ongoing research. We obtained a commitment from many of our residents and faculty for participation, and just purchased the devices to embark on our study with the start of the 2021-22 academic year. We look forward to sharing our results!
OHSU’s Department of Orthopaedics & Rehabilitation Thanks Dr. Jung Yoo for 15 Years of Service as our Chairman

By: Darin Friess, M.D.
Jung Yoo, MD, professor of Orthopaedics and Rehabilitation, OHSU School of Medicine, stepped down as Department Chair after 16 years on October 1, 2020. Dean Sharon Anderson noted that “He has been a staunch advocate for his faculty and never shied away from saying what he felt needed to get said... I, his patients and colleagues are grateful that he will remain on faculty.” During his tenure as chair from 2004 to 2020, Dr. Yoo developed a small Department into a leading force at OHSU, fulfilling all the facets of a successful academic practice, with managing 28 faculty and over 125 employees.
He grew up on the Northside of Chicago and graduated from Senn High School, which was most diverse public high school in the U.S., with students from 50 nations and 90% from families below the federal poverty level. He grew up working as a tutor, factory worker, and finally as finance clerk for the Chicago Tribune. At 18, he was baptized as a Roman Catholic and this became a guiding principle for his life. He graduated from Loyola University with a degree in biology, but spent much of his time studying philosophy, history, theology and economics - subjects he often quoted as Department Chair. Many a student, resident, fellow or staff will fondly recall a wide-ranging discussion of all these disciplines in answer to a simple question asked of Dr Yoo.
Dr. Yoo attended medical school at the University of Chicago. During this time period he met his lifelong love, Anne, on a Catholic Charities service trip. His devotion to Anne, his family, and his church have been a constant through his life. Later, a chance mentor during medical school at the University of Chicago turned him to a career in orthopedic surgery. He spent his residency at Case Western Reserve University and began a career in medical research that grew from the basic science of cartilage growth to innovation and one of the earliest patents on stem cells. While at Case Western, he developed an interest in spine surgery and chose to do a fellowship in nearby Syracuse, New York. As one might expect from Jung Yoo, he lived cheaply in New York and traveled back frequently to his family in Cleveland.
After his fellowship year he returned to the faculty at Case Western Reserve University to begin his academic career. During his time on faculty in Ohio, his surgical care was sought by patients and other physicians. He asked his patients difficult questions and used their answers to research problems faced after spine surgery. He wrote seminal papers on swallowing difficulties after cervical spine surgery and urinary retention issues after lumbar spine surgery, since these were details that mattered significantly to his patients.
Such academic successes led him to OHSU as a new Orthopaedic Department Chair after a national search in 2004. Under his leadership, the Orthopaedic Surgery Residency at OHSU expanded from 12 to 25 residents and he still found time to win the yearly resident teaching award. During his career he mentored over 40 fellowship trained spine surgeons. As chair at OHSU, he hired a faculty that provides high quality care and is devoted to education and research. He was an early advocate of the expansion of OHSU Health to reach the orthopedic needs of Oregonians “off the hill,” partnering with multiple institutions to build new clinical sites. He would proudly note that his department budget ran a positive fiscal margin every single year.
The many lives he touched to develop surgeons, educators, scientists, and genuine human beings is the legacy he leaves behind as a Department Chair. While Dr. Yoo will be moving on from the meetings and negotiations, he seems to relish the chance to return with greater devotion to his surgical practice and teaching. No doubt he will continue to make a difference for the patients he treats and the learners he teaches. As always, he will have a story to tell and a twinkle in his eye.
For his part, Dr. Yoo asked only to share his gratitude. “I would like to express my thanks to the department and OHSU for having confidence in me and giving me this opportunity of being the chair,” he said. “I am proud that the faculty and the residents in the department are consummate professionals dedicated to the mission of patient care, education and research. We have grown in all these areas and we work as one team that like each other and care for each other.”
In honor of Dr. Yoo’s impact on the lives of so many patients, staff, students, residents and fellows, the OHSU Foundation has opened The Jung Yoo, MD Endowment for the Advancement of Education and Leadership in Orthopaedics. In line with Dr Yoo’s legacy, this fund will be used to support the education and leadership of tomorrow’s orthopedic surgeons. The OHSU Department of Orthopaedics would encourage all who have benefitted from a quiet conversation to lifelong lessons from Dr Yoo to consider a donation. The fund can be located at https://www.ohsu.edu/ortho/giving-opportunities.