MR Defecography WO BODY Protocol
Last updated: 12/8/2023
Charge as: Pelvis WO
Scanner preference: 1.5T or 3T
Coil: Torso Coil
Scan time is approximately 30 minutes
- Patient Prep:
- Patient to empty bladder and rectum 1 HOUR before getting on table.
- Patient to undress from waist down. Provide patient with gown and adult diaper.
- Side table set up:
- Enema tip
- Three 60cc syringes filled with ultrasound gel
- Table & Positioning:
- Several chucks on table where patient’s buttocks will be.
- Torso coil positioned as you would for Female Pelvis exam.
- Patient will be supine.
- Headphones or a way to hear instructions during scanning / loud balanced dynamic scans
SCAN NOTES - Updated 12/8/2023
Instruct the patient on the various maneuvers they will perform with the dynamic scan prior to beginning the exam:
Rest
- Start the scan
- Tell patient Relax pelvic muscles as much as possible
- Stop the scan after 7-10 seconds of scanning
Squeeze (Kegel)
- Start the scan
- Tell the patient to squeeze (and hold that squeeze) for 4 seconds, and then relax for 4 seconds, and then squeeze for 4 seconds, and then relax for 4 seconds.
- Stop the sequence and start the Valsalva scan.
- Do not run this sequence twice.
Valsalva (Strain)
- Start the scan
- Tell the patient to strain for 4 seconds, and then relax for 4 seconds, and then strain for 4 seconds, and then relax for 4 seconds.
- Stop the sequence and start the Defecation scan.
- Do not run this sequence twice.
Defecation
- Tell patient to start defecation when they hear the scanner noise
- Start the scan
- The patient should start defecation.
- Tech watches the cine for defecation. For some people this can take some time and pushing and may last longer than the 200 frames, so you may have to repeat the sequence for a second attempt if no gel is expelled.
- If the patient expels the gel, continue scanning to watch secondary pushing efforts.
- After each attempt, ask the patient if they still feel like they have more to evacuate out.
- If they indicate that they have more to push out (or there is still a significant amount of gel still in the rectum), repeat the attempt with another sequence. This is because sometimes the most significant pathology is only seen after the rectum empties or after repeated pushing.
| Plane | Weighting | Slice | Gap | Fat Sat | FOV | Notes |
|---|---|---|---|---|---|---|
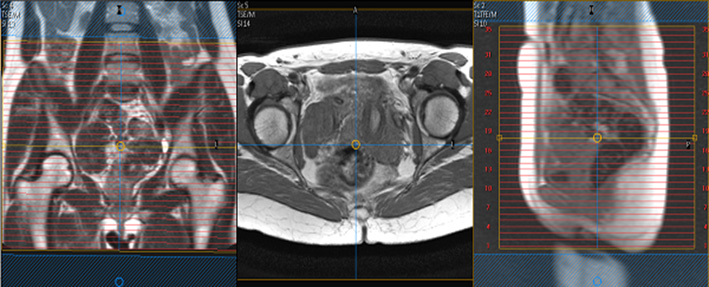
| Axial | T2 TSE | 5mm | 1mm | No | 200-240mm | Crest through entire perineum. TE 90-100, ETL 15, 2 NSA, Matrix 326-400 (can be lowered to accommodate scan time of 3-4min). |
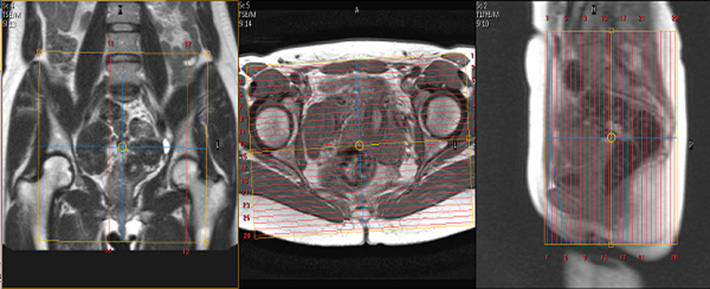
| Coronal | T2 TSE | 5mm | 1mm | No | 200-240mm | Sacrum to anterior abdominal wall, not necessarily skin to skin. TE 90, FOV 20-24, 5 skip 1, Freq. A/P, 2 NEX, matrix 326-400 |
| DYNAMICS | Single slice. Place in the midline through pubic symphysis and coccyx. Center lower anal /vaginal canal. | |||||
| Dynamic 1 (REST) | bTFE (Cine) | 7mm | - | - | 320-350mm | See notes for updated instructions |
| Dynamic 2 Squeeze (Kegel) | bTFE (Cine) | 7mm | - | - | 320-350mm | See notes for updated instructions |
| Dynamic 3 Valsalva (Strain) | bTFE (Cine) | 7mm | - | - | 320-350mm | See notes for updated instructions |
| Dynamic 4 Defecation | bTFE (Cine) | 7mm | - | - | 320-350mm | See notes for updated instructions |