Headache and Migraine Information for Providers

We know headaches are a top reason people seek medical care. Experts at the OHSU Brain Institute created this information to help you:
- Treat your patients.
- Decide when to consider imaging tests.
- Decide when to consider referring your patient to a headache specialist.
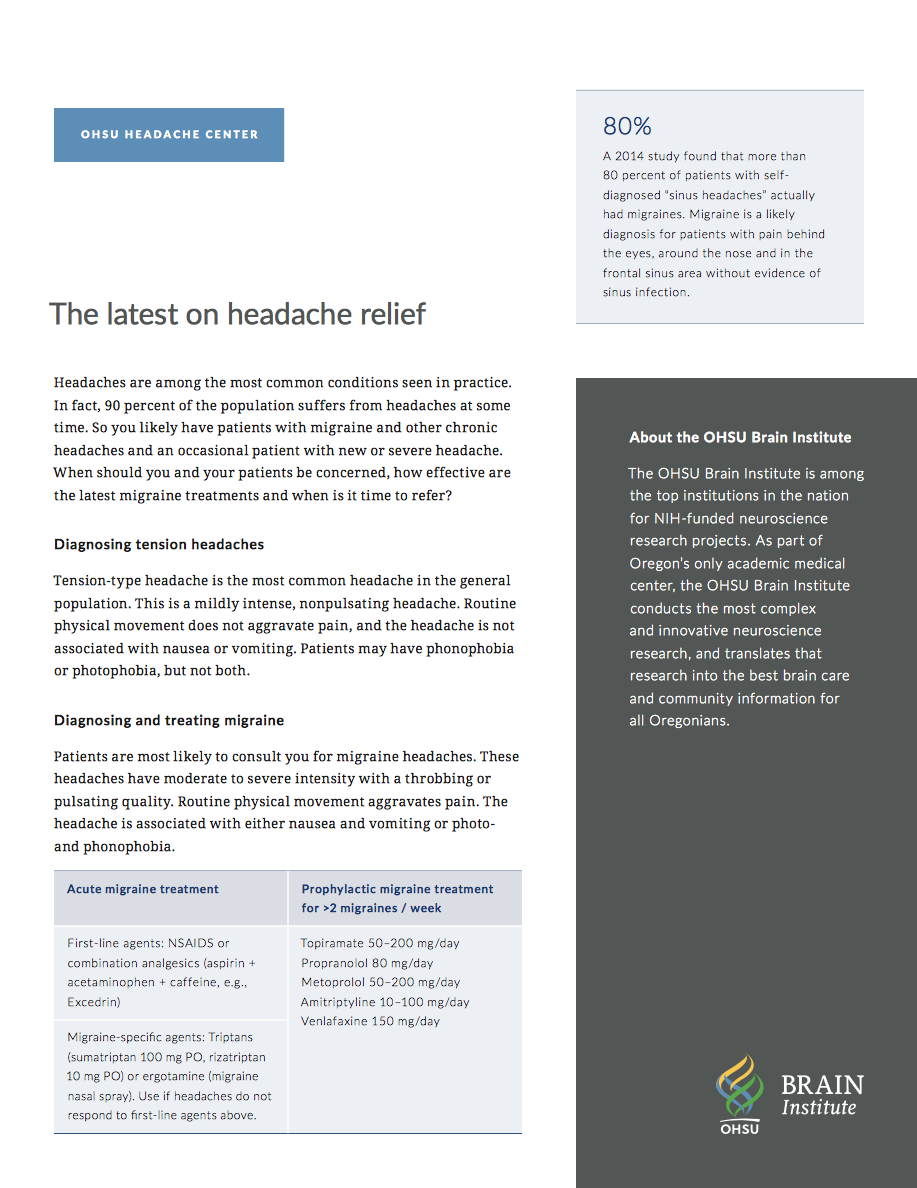
Diagnosing headaches
Tension headaches: This is the most common headache. It’s marked by mildly intense, nonpulsating pain. Routine physical movement does not worsen pain, and the headache is not associated with nausea or vomiting. Patients may be sensitive to light or sounds but not both.
Migraines: Patients are most likely to consult you for migraine headaches. These headaches have moderate to severe intensity with a throbbing or pulsating quality. Routine physical movement worsens the pain. The headache is associated with nausea and vomiting or sensitivity to light and sounds.
Is it a sinus headache or a migraine? A 2004 study found that more than 80% of patients who reported a sinus headache actually had a migraine. Absent evidence of a sinus infection, pain behind the eyes, around the nose and in the frontal sinus area indicates a migraine diagnosis.
Treating headaches
Tension headaches
These headaches are usually treated with over-the-counter medications that contain ibuprofen or acetaminophen.
Acute migraines
First-line agents: NSAIDS or combination analgesics such as Excedrin (aspirin + acetaminophen + caffeine)
Migraine-specific agents: If the headaches don’t respond to first-line agents, try one of these:
- Triptans (sumatriptan, 100 mg)
- Rizatriptan, 10 mg
- Ergotamine (nasal spray)
Preventive migraine treatment
These medications are appropriate for a patient having more than two migraines a week. Patients should be advised that prophylactic medication won’t prevent all their headaches. At best, medication alone can be expected to cut the number of headaches in half.
- Topiramate, 50-200 mg/day
- Propranolol, 80 mg/day
- Metoprolol, 50-200 mg/day
- Amitriptyline, 10-100 mg/day
- Venlafaxine, 150 mg/day
Migraine rescue plan
A sample rescue plan for a patient might include:
- Taking a dose of the medication that usually works well, such as rizatriptan.
- Taking a second dose if the headache is still present in two hours.
- Switching medications if the headache does not improve. A patient might switch from rizatriptan to high-dose ibuprofen or acetaminophen, for example, or to a different prescription medication, such as sumatriptan or DHE nasal spray (Migranal).
- Going to bed. Migraines frequently abate after a night’s sleep.
- Taking medication on awakening if the headache is still present. Call the office if the headache continues.
If the plan doesn’t work: We advise treating your patient with injectable medication in the office. Headaches that last to 48 to 72 hours can be extremely difficult to treat.
Tracking headaches
You can ask your patients to use a headache diary to record:
- The number of days (“headache days”) they have each month
- The intensity of each headache
- Medications used
Going over the diary at each visit can give you important information about whether current treatment is working. It also helps you prevent overuse of rescue medication.
Avoiding medication-overuse headaches
In one study, 60% of patients presenting to a headache center had medication-overuse headaches. In general, patients taking more than 10 doses a month of a rescue agent will have rebound headaches. Here’s a dosage guide:
Maximum monthly dosage
- Butalbital and combinations: Five tablets
- Opiates (such as Vicodin): Eight tablets
- Triptans or analgesics: 10 tablets
Note: Patients taking these medications for joint pain, lupus or other indications do not have rebound headaches.
Migraine, anxiety and depression
Patients with migraine headaches have four times the risk of anxiety and depression. It’s a two-way street: Patients with migraines tend to have anxiety and depression, and vice versa. Screening patients for depression and treating migraines with antidepressants can help both conditions.
Lifestyle changes and resources
A clinical trial showed that patients who get 40 minutes of aerobic exercise three times a week had fewer headaches than control subjects. We also advise patients to:
- Go to bed and get up at the same time each day.
- Avoid sleeping more than eight hours.
- Eat regular meals and snacks and to avoid skipping meals; patients with headaches are sensitive to drops in blood sugar.
- Drink at least 1.5 liters of water a day (50 ounces, or just over six 8-ounce glasses).
Our Headache FAQ and Resources page offers more information and tools for patients.
When to consider imaging
- Sudden onset of headaches
- Evidence of systemic illness such as fever, neck stiffness, weight loss, HIV infection, history of cancer
- New headache in patient older than 50
- Abnormal neurological signs such as weakness on one side or numbness
- Headache onset with vigorous exercise or sexual activity
- History of trauma
- Altered mental status
- Headaches worsen on observation
When to consider referring to a headache specialist
- Headaches no longer respond to rescue or preventive agents.
- Headaches occur more than twice a week or are severe enough to affect work, family and/or social life.
- Two preventive agents have failed.
- You’re not familiar with the headache presentation.
- You’re no longer comfortable managing the patient’s headaches.
Refer a patient
- Refer your patient to OHSU.
- Call 503-494-4567 to seek provider-to-provider advice.
Learn more
- Find more information on our Headaches and Migraines pages.
- Learn more about the OHSU Brain Institute, one of the nation’s top centers for NIH-funded neurologic research.