MR Female Pelvis for Uterine Cancer Staging WWO BODY Protocol
Last updated: 12/8/2023
Charge as: Pelvis WWO
Scanner preference: 1.5T
Coil: Torso Coil
- This is the Cervical Cancer protocol, except obliques are relative to the endometrium rather than the endocervical canal.
- Send ADC maps and subtractions
- FOV: do not include patient’s arms
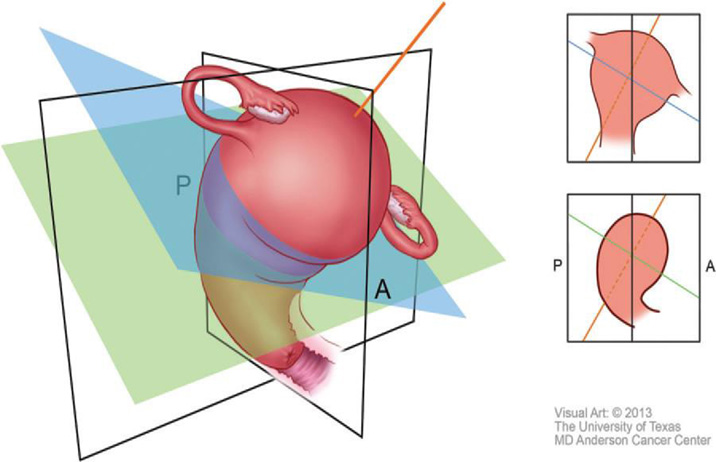
Figure 2. Obliques. Illustration shows a uterus that is ante¬riorly rotated in the sagittal plane (anteverted) and laterally tilted to the left in the coronal plane. The double oblique sequence is performed by an¬gling images anteriorly in the sagittal plane (green line) and laterally in the coronal plane (blue line), which creates true oblique images along the true axis of the uterus (orange line). A = anterior, P = posterior.
| Plane | Weighting | Mode | Slice | Gap | FAT SAT | FOV | Notes |
|---|---|---|---|---|---|---|---|
| COR | T2 | SSTSE BH | 5 mm | 1 mm | N | Large FOV to include kidneys. | Top of kidneys → pelvis . Sacrum → anterior abdominal wall. Pelvic pathology is often related to renal pathology. |
| SAG | T2 | TSE | 4 mm | 1 mm | N | 200-240 mm. Acetabulum → Acetabulum | If there is a pelvic mass, please scan to include the whole mass. Consider using an anterior Sat band if lots of abdominal wall motion. Matrix 256 x 256 |
| SAG | T2 | DWI | 4 mm | 1 mm | SPIR | B50, 500, 1000 | |
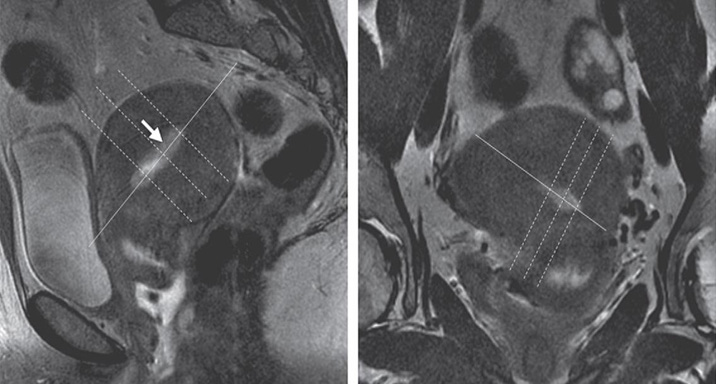
| AX OBLIQUE | T2 | TSE | 3 mm | 0.5 mm | N | 200-240 mm/ Fit to Patient. Uterus → rectum | Use all planes to obtain true axial of the endometrial canal (see images below). Matrix 512 x 256-512. Freq A-P. |
| AX OBLIQUE | T2 | DWI | 4 mm | 1 mm | SPIR | Match AX OBLIQUE | Trigger & track. Free-breathing sequence, so please position slices accordingly. B=50, 500, 1000. |
| AX | T1 | TSE | 5 mm | 1 mm | N | 200-240 mm/Fit to Patient. L5 → perineum | If there is a pelvic mass, please scan to include the whole mass. Freq A-P to avoid bowel motion ghosting into uterus and bladder. |
| AX | T2 | TSE | 5 mm | 1 mm | N | 200-240 mm/ Fit to Patient. L5 → perineum | Same parameters as AX T1 TSE. Freq A-P to avoid bowel motion ghosting into uterus and bladder. |
| SAG | T1 | 3D THRIVE precontrast | -- | -- | Y | Match SAG TSE T2. 240-280 mm | Non-high resolution THRIVEs. |
| Hand Inject Contrast | |||||||
| SAG | T1 | 3D THRIVE post contrast x3 BH | -- | -- | Y | Match SAG TSE T2. 240-280 mm | NON-high resolution THRIVEs. Perform at 30s, 60s, 90s post contrast. |
| AX OBLIQUE | T1 | 3D THRIVE HIGH RESOLUTION postcontrast | -- | -- | Y | Match AX OBLIQUE | HIGH RESOLUTION THRIVEs. |
| AX (True Ax) | T1 | 3D THRIVE HIGH RESOLUTION postcontrast | -- | -- | Y | Perineum to renal hila | HIGH RESOLUTION THRIVEs. |