At the forefront of corneal transplant surgeries, Winston Chamberlain, M.D., Ph.D., and the cornea team at Casey Eye Institute are redefining the landscape with new techniques and clinical trials.
The past 20 years have seen a paradigm shift in corneal transplant methodologies. “As early as the first decade of the 2000s, we were transplanting all five layers of the cornea to treat a failed back layer,” says Dr. Chamberlain.
This approach has since been refined to the fairly common approach of DMEK, or Descemet’s membrane endothelial keratoplasty, which transplants a single cell layer. Today, DMEK is the standard method of corneal transplant for routine cases. However, since the procedure is challenging to learn, Dr. Chamberlain is working with corneal fellowship directors from across the United States in his role as advisory board chair of the Eye Bank Association of America, encouraging all trainees to learn DMEK in their specialty training.
DSO for Fuchs dystrophy
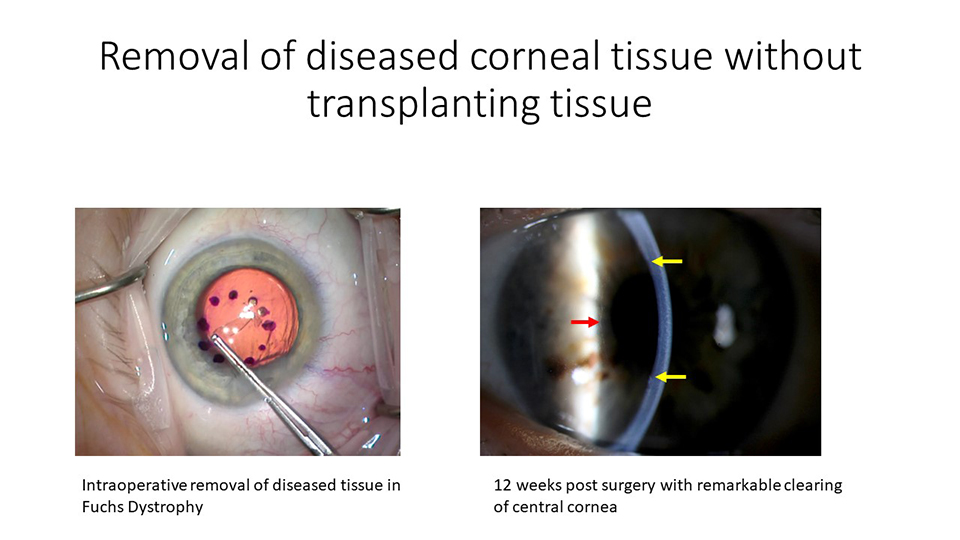
Now, Dr. Chamberlain and other investigators are studying two new ways of replacing damaged corneal tissue in clinical trials. The first uses a technique called DSO, or Descemet’s stripping only. Used primarily for patients with Fuchs dystrophy, it involves removing only the cells with characteristic granular bumps, called guttae, found in Fuchs.
The next step is using a rho-kinase inhibitor (Ripasudil hydrochloride hydrate, or Glanatec,®; Kowa Company Ltd., Nagoya, Japan) to block cell death and encourage endothelial cells to spread, Dr. Chamberlain explains. The use of rho-kinase (ROCK) inhibitors allows healthy peripheral cells to fill the space where damaged tissue was removed.
Since patients’ own cells replace those removed, the risk of rejection – a common problem with corneal transplants – is no longer a concern. So far, DSO works well for some patients. If not, patients receive a corneal transplant, usually with DMEK.
New and newer: DMEK vs. DSO
The DETECT-2 trial is an NIH-sponsored study co-designed by Dr. Chamberlain and colleagues from the University of California, San Francisco, and Byers Eye Institute at Stanford University. It compares the use of DSO and DMEK and explores the potential of ROCK inhibitors to prolong graft life and reduce failure rates. The trial is currently enrolling patients.
“At Casey, we have increased our frequency of clinical trial participation in the last half decade or so,” Dr. Chamberlain says. “We plan to continue to help design, select, and be involved in developing the treatments most relevant to patient care in Oregon, as well as to have a worldwide impact on the science.”
Cellular therapies, the next frontier
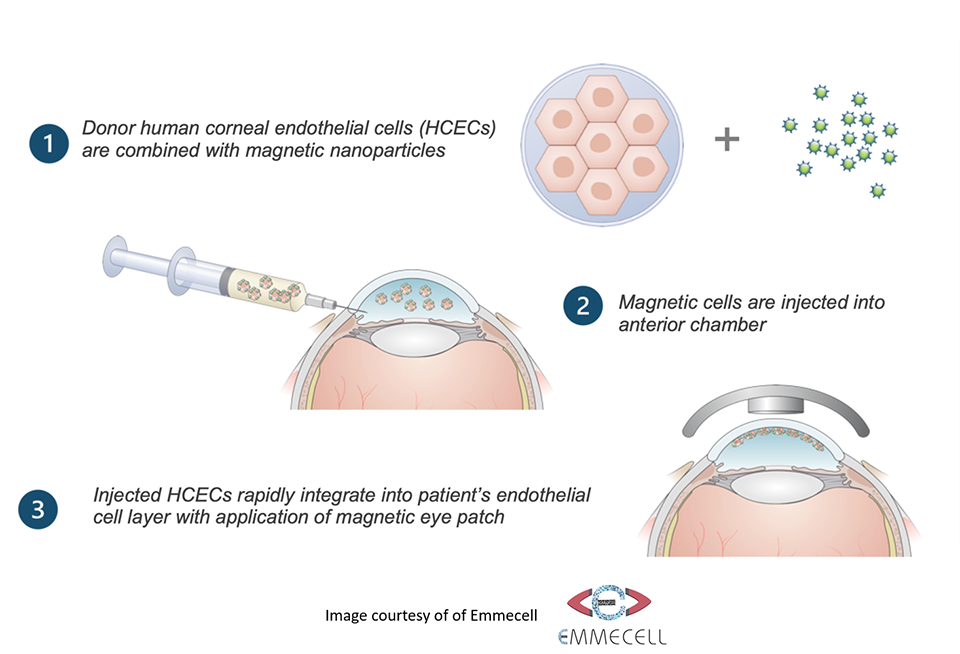
The vision for new therapies extends to making the most of every donated cornea. In another clinical trial, endothelial cells from a single donor cornea are enhanced with microscopic magnetic beads before being injected into the eye. A magnetic eye patch draws the new cells forward to the corneal surface. Over three or four weeks, the cells spread to cover the back of the cornea.
Preliminary signs of success come from a small pilot trial of approximately 15 patients in Mexico. “We are one of fewer than a dozen centers for this trial,” says Dr. Chamberlain. “The first patient is scheduled to be treated here in late 2023.” With this technique, a single donated cornea can help more than one person regain sight – the potential is there to help dozens or even hundreds of people with vision loss.
The minimally invasive injection procedure takes about three minutes, with fewer complications compared to regular DMEK or DSEK surgery.
A similar trial of an approach without magnetic beads involves slightly different corneal preparation. “Heterogeneous approaches are a good idea,” Dr. Chamberlain says. “They can provide options for patients with different manifestations of corneal disease.”
Global impact spreads beyond Casey
All of these developments can help close the enormous gap between supply and demand for corneal therapies, especially in underserved regions.
“One paper suggested that in the last 10 years, approximately 13 to 15 million people have become blind from repairable corneal injury or disease,” says Dr. Chamberlain. However, only about 180,000 corneal transplants are done globally each year.
The impact also tends to span more years than the impact of age-related vision loss. “People with corneal injuries or dystrophies tend to become blind at younger ages and live longer with the loss of function,” Dr. Chamberlain says.
With regular use of cultured endothelial cells, fewer people in regions like Africa and Southeast Asia, where most people lack access to eye bank tissue, would lose their sight
Dr. Chamberlain's vision and the role of Casey Eye Institute
Dr. Chamberlain's enthusiasm is palpable when discussing the future of corneal transplants. "Even if we end up doing less surgery and more fine-tuning, we will have more options available for patients, including those who cannot tolerate conventional transplantation," he says. Under his guidance, the Casey Eye Institute has become a hub for innovation and excellence in corneal transplant.
The institute's success in these trials, particularly DETECT-2, is a testament to its commitment to advancing corneal transplant technology. By being involved in these cutting-edge trials and collaborations, Dr. Chamberlain and his team at Casey Eye Institute are not just witnessing the future of corneal transplants; they are actively shaping it.
Their work exemplifies the rapid advancements in the field, and their dedication to innovation, patient care, and scientific research is paving the way for treatments that not only transform patient outcomes but fundamentally change the way we approach corneal health and vision restoration.