Evaluating Immunotherapy-induced Adverse Cutaneous Events
Overview
Immunotherapy, or immune checkpoint blockade (ICB), works by using the patient’s own immune system to kill cancer cells. These types of drugs have been successful in treating various cancers, including melanoma. However, these therapies can cause the immune system to attack healthy tissue causing immune related adverse events (irAEs). These side effects can result in an adverse cutaneous event (rash) in 30-65% of patients on ICB therapy and this can lead to discontinuing a lifesaving treatment.
The immune microenvironment in the skin is not very well characterized and less is known about how this environment changes with ICB therapy or why some patients develop ICB-induced rashes. If we can uncover common immune-associated pathways within rash samples we can more precisely target the inflammation associated with the rash and not have to interrupt ICB therapy or place the patient on broad immunosuppressive drugs, like steroids.
Research
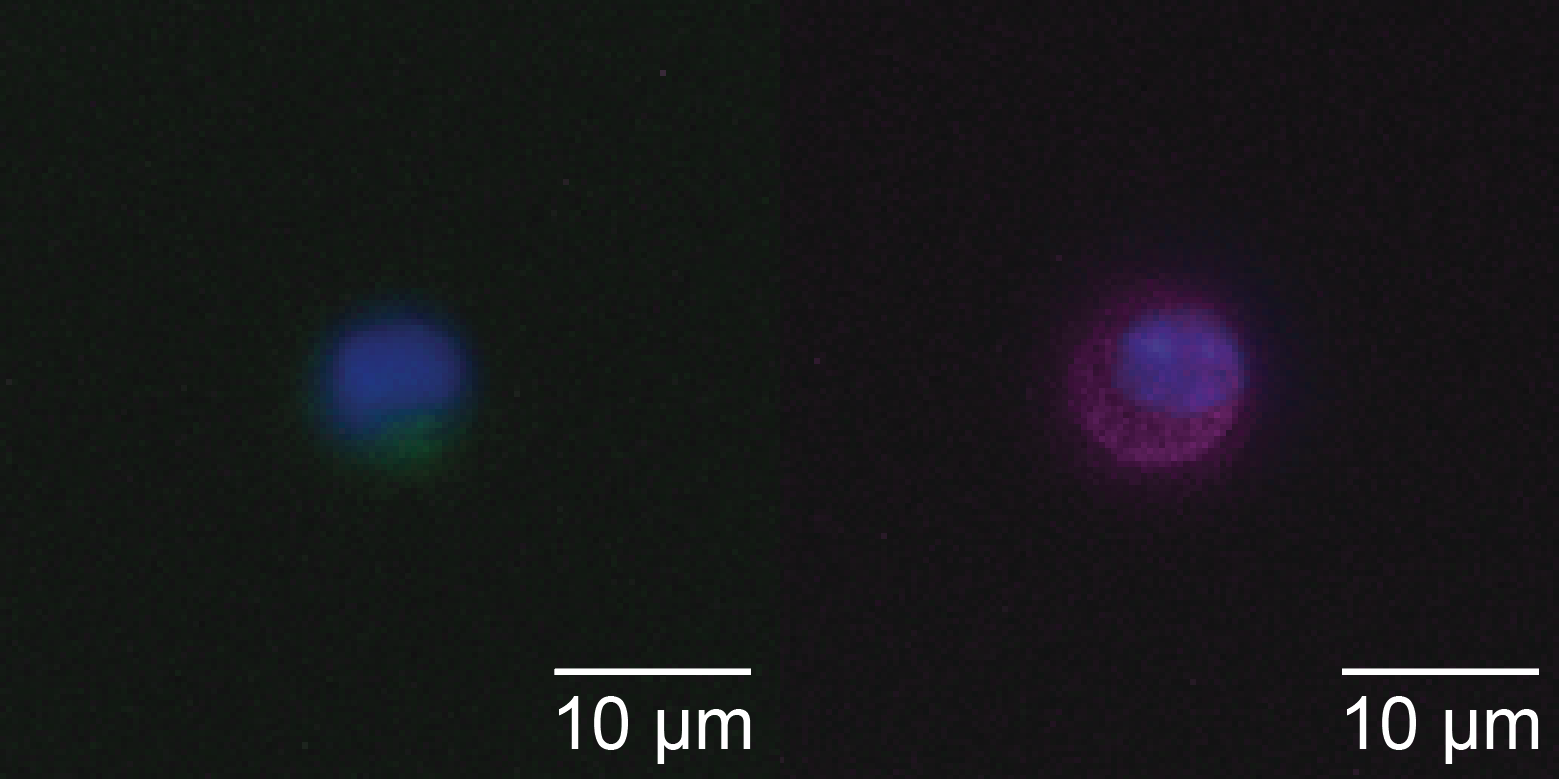
The Kulkarni lab takes skin and blood samples from patients prior to starting ICB therapy, if they develop a rash, and 12 weeks after starting therapy. We use some of the skin sample to breakdown and isolate the immune cells within the skin and run single cell RNA-seq and protein analysis using Ab-seq on the same cell. This gives a picture of what types of immune cells are in the skin at various stages prior to and during treatment. We take the rest of the skin sample and make a tissue block to create tissue sections to preform multiplex immunohistochemistry (mIHC) that allows for spatial resolution of the immune cells within the skin and ICB-induced rashes.
The blood samples are stored as plasma and the PBMC fractions which can be interrogated later to see if common biomarkers are present in the skin and the blood of patients that develop rashes.