Voice & Swallowing - Problems/Disorders
The following pages discuss the symptoms, causes, and treatment for some of the more common voice and swallowing (larynx-related) disorders. Note: The information contained in these pages is for educational purposes only. It should not be construed as individualized diagnostic and treatment advice.
Select a Disorder Topic
Laryngitis
Spasmodic Dysphonia
Vocal Fold Impairment
Polyps
Cysts and Nodules
Contact Granuloma / Contact Ulcer
Laryngeal Cancer
The Aging Larynx
Parkinson Disease
Paradoxical Vocal Cord Dysfunction (VCD)
Chronic Cough
Swallowing Disorders (Dysphagia)
Zenker’s Diverticulum
Laryngitis
Laryngitis, or inflammation (swelling) of the larynx, is probably the most common problem with the larynx and voice. This inflammation may be by itself, or a symptom of another problem. Laryngitis can be acute (short-term) or chronic (long-term).
Symptoms: The usual symptoms of laryngitis are hoarseness and loss of voice. Occasionally, laryngitis may cause pain in the laryngeal area during swallowing or speaking.
Causes: Laryngitis can have many causes. Acute laryngitis frequently accompanies viral or bacterial upper respiratory tract infections. Long-term laryngitis can have a number of causes. Among the most common are misuse or overuse of the voice and irritation by smoke, dust, or other airborne irritants. Reflux of acid from the stomach is another frequent cause of laryngeal inflammation. Laryngitis can be a symptom or a side affect of a more serious condition such as benign or malignant growths. Therefore, if hoarseness lasts longer than two weeks, or is accompanied by a lump in the neck or blood-tinged spit, you should see a doctor.
Treatment: Acute laryngitis is treated with resting the voice as much as possible, increasing intake of decaffeinated fluids (particularly water), and using a humidifier. If a bacterial infection is the suspected cause, antibiotics may be prescribed. Chronic laryngitis is treated differently, depending on the cause. As mentioned above, if symptoms persist for longer than two weeks or if common treatments are ineffective, seek medical advice.
Return to top of Page
Spasmodic Dysphonia
Spasmodic Dysphonia (SD) is one of a group of neurologic disorders called dystonias. A dystonia is a movement disorder characterized by inappropriate contraction (tightening) of muscle groups. With SD, the laryngeal muscles are involved. There are two primary types of SD. The most common type is adductor SD. This occurs when the muscles which close the vocal folds (thyroarytenoids and lateral cricoarytenoids) contract with excess force. Abductor SD involves the muscles which open the vocal folds(posterior cricoarytenoids). A "mixed" form involving both the abductor and adductor muscles also exists.
Symptoms: The symptoms of SD depend on which form is present. The adductor type produces a strained or strangled voice quality. Abductor SD usually produces a breathy and effortful voice. Both types cause abrupt breaks in sounds and makes the voice harder to understand. Voice is often worse on the telephone or when the speaker is under stress. Some voice production can be normal, such as laughing, coughing, and singing.
Causes: The precise cause of SD is unknown and may involve multiple factors. It does appear to be a neurological (not psychiatric) disorder, similar to other focal dystonias.
Treatment: Currently, the most effective treatment for SD is injection of botulinum toxin - type A (Botox). Botox is injected into the laryngeal muscles via the neck (just under the adam's apple) using EMG guidance or through the mouth using a special needle that curves over the tongue. Botox interferes with the muscle contractions and prevents the spasms associated with SD. Botox treats the symptoms of SD, but it does not cure the disorder. The effects of Botox injections are usually apparent within 24 hours and last for four to six months. Risks and discomfort during the procedure are minimal.
After an injection for adductor SD, patients may experience a weak, breathy voice and mild difficulty swallowing for one to two weeks. Voice therapy is used in conjunction with Botox injections to maximize voice capabilities during the breathy period, minimize the dysfunction as the spasms return, and lengthen the time between injections.


Return to top of page
Vocal Fold Motion Impairment
The vocal folds, because of the position in the airway, play a vital role in speech, swallowing, and breathing. In order to perform these functions normally, the laryngeal muscles must be able to abduct (open) and adduct (close) the folds.
Vocal fold motion impairment is of two major types: unilateral (more common) and bilateral. These types differ in their seriousness, symptoms, and treatment.
Symptoms: Patients with unilateral paralysis may have a weak and "breathy" voice, and speaking may require considerable effort. Because the vocal folds are unable to close completely during swallowing, patients may also experience coughing and choking while eating or drinking. Patients with bilateral paralysis may experience these symptoms, but the possibility of a compromised airway is a more serious threat. The muscles which normally abduct the folds and provide for a patent airway are unable to function. Thus, the folds may remain adducted in the airway and block normal breathing.
Causes: The most common cause of vocal fold motion impairment is injury to the recurrent laryngeal nerve, the nerve responsible for controlling the main muscles of the larynx. This may be due to injury, surgery, viral infection, a tumor pressing on the recurrent laryngeal nerve, or other causes. Occasionally, injury or diseases of the brain, including stroke, result in impaired motion.
Mechanical obstruction (problems with the muscles or cartilage around the larynx) can also result in vocal fold motion problems. The arytenoid cartilages can become "locked" and restrict movement. Scar tissue may also accumulate and inhibit vocal fold movement.
Treatment: A combination of surgery and voice therapy (see the Rehabilitation page for more information on voice therapy) is used to treat unilateral motion impairment:
In the patient with unilateral impairment, the left vocal fold fails to move at the same time as the right fold. These patients will also experience hoarseness and loss of voice quality. In the patient with bilateral vocal fold motion impairment, the vocal folds remain adducted (closed) at the midline and movement is minimal. This can lead to airway compromise and restriction of breathing.
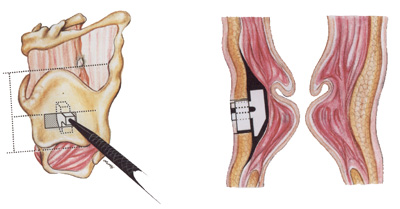
Medialization thyroplasty is a surgical procedure in which a small cut is made in the skin near the larynx and a small piece of thyroid cartilage removed. A small block, usually made of silicone or hydroxylapatite, is secured in the cartilage. This block acts as a shim which pushes the vocal fold in the middle, helping to improve vocal fold closure. This procedure is relatively quick and painless and is usually performed under local anesthesia.
The images below show the medialization thyroplasty procedure. The image on the left shows the placement of the shim in the thyroid cartilage. The image on the right demonstrates how this shim, when correctly placed, can help push a motion-impaired vocal fold medially.
The second treatment for unilateral vocal fold motion impairment involves the injection of small amounts of materials directly into the vocal fold. Again, the goal is to push to fold in the middle and restore function. This technique, while effective, is limited by the difficulty of controlling the placement and volume of the injected material.
Voice therapy is useful when the vocal folds can almost close. Therapy techniques are designed to improve voice quality, increase loudness, and lessen the feeling of running out of air when talking. Therapy is often used to "fine-tune" the voice after surgery, with goals of decreasing any left over "gravelly" quality and vocal fatigue.
Several options exist for the treatment of bilateral vocal fold motion impairment. All of these treatments seek to improve breathing, but have different effects on the balance between breathing, voice quality, and airway protection during swallowing. In some cases a tracheostomy may be required. It is a commonly performed procedure where an opening between the neck (below the level of the vocal folds) and the trachea is created surgically. A transverse cordotomy is another option and involves removing a small portion of the vocal fold from one or both sides.
Newer procedures for dealing with bilateral vocal fold motion impairment have recently emerged. One of these, a posterior cricoid split, involves splitting the cricoid cartilage and inserting a cartilage graft. This allows for a larger glottal opening and can help to relieve the symptoms of vocal fold motion impairment. An even newer technique, laryngeal pacing, involves the implantation of a small device which causes coordinated abduction of the vocal folds during respiration.
Return to top of Page
Polyps
Polyps are benign (non-cancerous) lesions that usually develop at the junction of the front and middle third of the vocal fold edge. They may appear as pedunculated (attached by a slim stalk) or sessile (closely adhering to the mucosa). A variant of these types is the hemorrhagic polyp, which has the appearance of a blood-filled blister on the vocal fold surface.
Symptoms: Typical symptoms of polyps include hoarseness, breathiness, or vocal roughness. These signs are commonly accompanied by the sensation of something in the throat.
Causes: Polyps are thought to result from vocal abuse and misuse. They are often associated with a single traumatic event (such as yelling at a sports event), but can be the result of prolonged vocal abuse.
Treatment: Polyps are usually surgically removed under general anesthesia. Following removal, limited voice use is recommended for a minimum of two weeks. Voice therapy is also commonly implemented to facilitate healing and minimize the potential for recurrence.
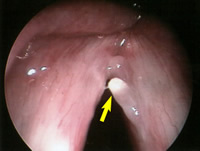
The image below is a magnified view of a vocal fold polyp (yellow arrow).
Return to top of page
Cysts and Nodules
Vocal fold nodules and cysts are benign (non-cancerous) growths which can affect people of all ages. While the symptoms of cysts and nodules are similar, treatment usually differs. Cysts and nodules also differ in the location on the vocal fold. Nodules are most often found on both sides of the folds, and are found at the junction of the front and middle third of the free edge of the vocal folds. Cysts are usually only found on one side and can occur anywhere on the fold. When the cyst is at the free edge, it is common for a reactive nodule to form at the same location on the other fold.
Symptoms: The most common symptom of nodules and cysts is hoarseness. Voice production is often hard, and takes effort. Occasionally, a growth will become large enough to cause pain.
Causes: Nodules typically occur as a result of voice misuse or overuse, which causes irritation and inflammation of the vocal fold mucosa. With continued misuse, the tissue becomes hardened. Cysts, on the other hand, are usually the result of a blocked mucous gland within the fold. As mucous fills up the area behind the blockage, the tissue grows and swells, and a cyst is produced. There appears to be a link between cysts and voice misuse, especially when nodules occur in the same location. Some cysts occur at the time of birth and may show up with symptoms years later.
Treatment: Vocal nodules are generally treated with voice therapy. The patient is taught voice production techniques to decrease the contact force between the nodules. Voice therapy also teaches the patient to avoid behaviors which might cause or aggravate the nodules. Some medical conditions (such as allergies and laryngo-pharyngeal reflux) can maintain the presence of the nodules and require treatment. In some instances, surgery is necessary to remove the nodules. In these cases, pre- and post- operative voice therapy is also used. Cysts are treated primarily by surgical removal, with voice therapy is often used to decrease swelling from surgery and to improve voice quality. Therapy is also used to treat any reactive nodules. Although it is possible the cysts or nodules will return, treatment for both nodules and cysts is usually successful and normal voice function returns.
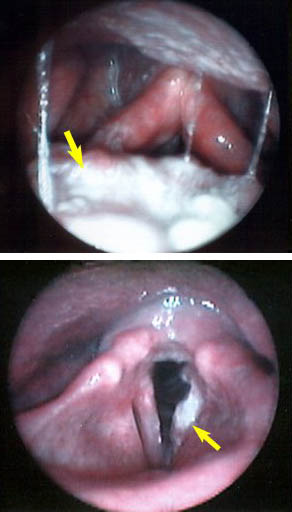
The image below is a laryngoscopic view of vocal fold nodules (yellow arrows).

Return to top of page
Contact Granuloma/Contact Ulcer
Contact granulomas or contact ulcers are formed as a result of injury to the delicate tissues of the larynx. In response to this trauma, the mucosa of the vocal folds either ulcerates, forming a contact ulcer, or produces a heaped-up bunch of tissue, a contact granuloma. These lesions usually appear as a build-up of pinkish-white tissue near the cartilages at the rear of the larynx.
Contact granulomas occur almost always in males over the age of 20. They are common in professional voice users such as lawyers, ministers, business executives, and physicians.
Symptoms: The primary symptom of a contact granuloma is the sensation of a foreign body in the throat. Constant and vigorous throat-clearing is often present and, less often, hoarseness or a husky-sounding voice. Pain, usually described as sharp and stabbing, may also be present and may radiate toward the ear.
Causes: Contact granulomas are commonly caused and maintained by a combination of laryngopharyngeal reflux, voice misuse, and excessive throat-clearing or coughing. These activities cause the vocal folds to "slap" together forcefully, traumatizing the mucosa. Granulomas can also be caused by direct injury to the vocal folds, for instance as a result of intubation.
Treatment: Inhaled steroids and an antireflux regimen are generally the initial treatment. After the first (initial) treatment, voice therapy is commonly used to teach the patient to avoid those behaviors which may injure the vocal folds. Surgery to remove these types of lesions is usually undertaken as a last resort because the problem usually happens again.
Return to top of Page
Laryngeal Cancer
Like all cancers, laryngeal cancer is the result of uncontrolled division by the body's cells. As these cells divide and build up, a mass develops. Unlike benign growths, however, cancer can invade healthy tissue and spread to other parts of the body. This process is called metastasis, and it is the reason why it is important to identify cancers early.
Symptoms: The symptoms of laryngeal cancer depend largely upon the size and location of the tumor. Hoarseness or other changes in vocal quality are often the first symptoms. Large tumors may interfere with the airway and cause difficulty breathing or noisy breathing. Tumors can also cause difficulty swallowing. Other symptoms may include throat or ear pain, lumps in the neck or throat, blood in the spit, or a persistent cough.
Causes: The exact cause of cancer is unknown, but the risk factors are well established. Cancer of the larynx usually occurs in patients over the age of 55, and is four times more likely to occur in men than in women. It is also more prevalent in the African-American population than in the Caucasian population. Smoking, especially with heavy alcohol consumption, also increases the risk of cancer. Exposure to carcinogens in one's environment (e.g. asbestos) is also associated with laryngeal cancer.
Treatment: The treatment for cancer of the larynx depends on the size and stage of the tumor, as well as the age, health, and opinions of the patient. Treatment usually involves radiation therapy, chemotherapy, surgery, or a combination of these methods. The images below show laryngoscopic views of laryngeal tumors (yellow arrows). The image on top is of a large supraglottic tumor.
In radiation therapy, high-energy rays are directed at a tumor and the surrounding tissue to stop the cancer and prevent its spread. Radiation therapy usually lasts five days a week for five to six weeks. At the end of this period, the tumor bed often receives an additional "boost" of radiation. Some individuals may receive chemotherapy at the same time as their radiation treatment or separately. This involves taking a chemical agent which slows the growth and multiplication of the cancer cells and may increase the likelihood of a cure with either surgery or radiation treatment.
For larger tumors, or if radiation therapy or chemoradiation has failed, surgery may be indicated. A partial laryngectomy may be performed, in which only a portion of the larynx is removed. This has the advantage of preserving the voice, although in many cases swallowing therapy is required for a ongoing period in order for the individual to resume eating and drinking. If a tumor is widely invasive, however, a total laryngectomy may need to be performed in which the entire larynx is removed. The pathways for breathing and swallowing have to be separated once the larynx is removed and therefore, at the time of surgery, a permanent opening in the neck is made which is known as a “tracheostoma” or “stoma”. The stoma is typically about the size of a nickel or a quarter. Because a total laryngectomy includes removal of the vocal folds, normal voice is no longer possible. However, alternate speech techniques are possible. If a surgeon suspects that cancer may have metastasized (spread) to nearby tissue, a radical neck dissection may also be performed to remove the lymph nodes and surrounding tissues in the neck.
Return to top of Page
The Aging Larynx
The larynx, like any other part of the body, changes as we grow older. Many of these changes are not noticeable; however, some of the changes can affect the quality and sound of the voice. The framework cartilages of the larynx turn to bone, which is less flexible, and the cartilages responsible for vocal fold movement become less flexible/mobile. Over time, the fibers that help the vocal cords work (tighten and relax) become thicker and less flexible. These changes, along with changes in the elasticity (flexibility and stretchiness) of the vocal folds and changes in brain control of those muscles, affect how voice production happens, usually with a decrease in control. Voice can become breathy, rough, hoarse, and more quiet as we age. The pitch of the of the voice tends to lower for women and rise for men. We can use special video equipment to see the changes in the muscles and fibers of the folds for diagnosis and treatment.
A program of voice therapy exercises is often helpful in maintaining or restoring some of the muscle function and improving voice quality and projection (loudness). If needed, there are surgical procedures available to improve vocal fold closure.
Return to top of page
Parkinson's Disease
Parkinson disease is a movement disorder that causes muscle rigidity, slow movement, stooped posture and tremors. There is no known cure for Parkinson disease but there are several medications and medical treatments used to treat the symptoms. Although conventional medical treatments typically improve limb function and reduce tremor, these treatments do not significantly improve voice and speech function.
Current research shows that at least 89 percent of people with Parkinson Disease experience communication problems that may include reduced loudness, monotone pitch, breathy voice quality, hoarse voice quality and/or slurred speech. As a result of these communication problems, people with Parkinson disease report that they are less likely to participate in conversations, are less outgoing, and feel left out of conversation. They feel that they have less confidence in social settings. People can no longer hear them or understand them.
Why do people with Parkinson disease experience reduced loudness, monotone pitch, or a hoarse or breathy voice? There are several reasons that these changes occur. Parkinson disease affects how the body can move, which means people with Parkinsons move more stiffly and slowly and have tremors. Changes in the brain results in reduced muscle activation which leads to bradykinesia (slow movement) and hypokinesia (small movements). This decrease in muscle activation can result a decrease in systems related to speech including respiration (breath support), laryngeal function (voice and loudness) and articulation (clarity of speech). Lee Silverman Voice Treatment is a therapy program designed specifically for individuals with Parkinson Disease who are experiencing these problems.
Return to top of page
Paradoxical Vocal Cord Dysfunction (VCD)
Paradoxical vocal cord dysfunction or VCD is a condition which leads to shortness of breath or stridor (high pitched or gasping sounds coming from the throat). VCD is often mistaken for asthma, but it does not typically respond to asthma medications. Often the person with VCD feels as if their airway is closing or partially closing and is to get air in. In some cases the throat feels squeezed tight on both breathing in and out. During normal breathing, the vocal cords, which sit at the top of the airway, open to allow air to flow freely in and out of the lungs. During a VCD attack, the airway becomes temporarily narrowed due to the vocal cords partially blocking the airway. The shortness of breath is caused by movement of the vocal cords toward each other during the breathing cycle. VCD often occurs in teenage athletes, but can occur at any age. In adults, the symptoms are most often triggered by environmental irritants. There are often feelings of panic and anxiety associated with the attacks due to the sensation of being unable to breathe. Though the sensation of not being able to breathe is very frightening, VCD is typically a functional disorder and may successfully respond to treatment.
The primary symptom of VCD is shortness of breath. There is usually a feeling of tightness in the upper chest and/or throat area when it occurs. There is often more difficulty breathing in than breathing out. VCD can occur with asthma (in as many as 40% of the cases) making the diagnosis more complicated. Because the vocal cords are drawn together during a VCD attack, coughing, stridor (noisy breathing) and difficulty talking may occur. VCD symptoms usually come on fairly suddenly, often during exercise or after exposure to an irritant. The symptoms usually subside anywhere from 2-30 minutes after the exercise or exposure has been stopped. Between attacks, individuals typically breathe normally and do not feel short of breath. There are some individuals with VCD, however, who report a consistent feeling of constriction in the airway and shortness of breath throughout the day.
There is not usually a single obvious cause leading to VCD. Rather, there are usually a number of factors that may add to the problem. Anything that can be an irritant to the vocal cords and upper airway can contribute to VCD. This would include gastroesophageal reflux disease which may cause acid to spill into the laryngeal area, irritation from ongoing allergies, or exposure to inhaled irritants (e.g. smoke, toxic chemicals, and perfumes). Stress or anxiety may also contribute to the problem. The most common trigger of VCD in adolescents is hard exercise.
Any breathing difficulty should first be evaluated by a physician. A pulmonologist or asthma allergy specialist can diagnose whether asthma is present. The best way to confirm VCD is by doing laryngoscopy to look at the vocal cords, during an attack if possible. Laryngoscopy is an examination which is conducted in the ENT clinic and allows the doctor to see the larynx or voice-box with a special camera. Laryngoscopy can rule out any physical problem with the larynx as well as identify abnormal vocal cord motion during breathing. Some asthma and allergy specialists are able to do this, as are otolaryngologists (ENT doctors) and some speech pathologists. In specialty clinics such as ours at OHSU, we will often try to trigger an attack so that we can view what happens to the airway when this occurs. The examination is recorded so that the individual with VCD can be taught about the vocal cords and how it workss. VCD often responds very well to therapy and is treated by the voice therapists in the ENT clinic.
Return to top of page
Chronic Cough
Individuals with chronic cough and throat clearing may also be referred to the NW Voice & Swallowing Clinic. Usually, these individuals have already had an extensive work-up of their condition and other causes of cough have been ruled out. Chronic cough or throat clearing may be caused by ongoing irritation of the larynx. The cough and throat clearing typically tend to make that irritation worse but have become habitual, so breaking the pattern is an important part of alleviating the cough. There are some medications which can help to decrease the sensitivity in the larynx and therefore help to decrease the cough. Behavioral treatment by a speech therapist can be helpful in decreasing the frequency and severity of coughing and throat clearing. Treatment often starts with looking at the larynx to rule out any anatomic abnormality. Then the individual is taught strategies to decrease throat clearing and specific breathing strategies for avoiding or interrupting cough can be taught. These strategies often prove to be very helpful in decreasing the frequency and severity of chronic cough and throat clear.
Return to top of page
Swallowing Disorders (Dysphagia)
Swallowing is defined as the passage of food or liquid from the lips to the stomach. Swallowing problems, or dysphagia, include any problem with that process. Typically, the process of swallowing is divided into several phases:
- An oral phase during which the food or liquid is prepared and moved from the mouth to the throat
- A pharyngeal phase during which the airway closes and the food or liquid is moved from the throat and into the esophagus
- An esophageal phase during which food or liquid then passes along the esophagus and into the stomach
Common oral and pharyngeal swallowing problems may include the following:
- Choking
- Feeling as though food or liquid hangs up in the throat
- Frequent coughing before, during or after eating
- Difficulty managing saliva
- Frequent respiratory infections or pneumonias
- Wet vocal quality (sounding as though the voice is “underwater”)
- Avoiding foods or liquids that were previously eaten
- Increased mealtimes
- Weight loss
- Regurgitation (throwing up) of food after swallowing
You should have a doctor check on you if any of these symptoms are new, unexplained or appear to be getting worse. Oropharyngeal swallowing problems may be diagnosed by an otolaryngologist, speech pathologist, radiologist, neurologist and other medical specialists.
Oropharyngeal dysphagia, or swallowing difficulty, is associated with high levels of illness, death, and cost. The most common cause of adult dysphagia is stroke, but other diagnoses include Parkinson’s disease, ALS, multiple sclerosis, muscular dystrophy, head and neck cancer, myasthenia gravis, prolonged intubation, and other surgical procedures. It has been estimated that 300,000 to 600,000 individuals each year are affected by dysphagia resulting from neurologic disorders. Regardless of the cause of the swallowing disorder, individuals with dysphagia are at high risk for malnutrition, respiratory infection and death. In the United States, hospitalisation for aspiration pneumonia nearly doubled in the period from 1991-1998 making it the second most common reason for hospitalization. Treatment for dysphagia is often multidisciplinary and may involve physicians, nursing staff, a dietician, and a speech pathologist, as well as the individual with dysphagia and the family or caregivers.
Return to top of page
Zenker's Diverticulum
A Zenker’s diverticulum is a when a small pocket or pouch forms at the border between the throat and the esophagus. There is a muscle which these two areas and which allows food and liquid to move downwards when swallowing but tightens to prevent regurgitation of the swallowed material and any reflux from reaching the throat. Within the fibers of this muscle, a small pouch can form then gradually gets bigger over time. Consequently the diverticulum is often not identified until later in life.
Symptoms associated with a diverticulum include regurgitation (throwing up) of foods and liquids after swallowing, pills becoming lodged and dissolving in the throat causing a bad taste, bad breath, and in some cases choking and even aspiration when reclined. In most cases a Zenker’s diverticulum is not life-threatening but they do tend to increase in size over time, causing a gradual worsening of symptoms. There are a number of surgical options for a Zenker’s diverticulum. These surgeries aim to cut part of the wall of the pouch which will then allow material to empty into the esophagus more normally. The decision about which surgical method to use is usually made based upon a number of factors including the size and location of the diverticulum, its accessibility and an individual’s overall health. These options will usually be discussed with you by your surgeon.
Return to top of page
How to Make an Appointment
Please contact our office regarding scheduling appointments. Prior to scheduling an appointment, our providers often need to review chart notes related to the reason you want to be seen in order to coordinate any additional tests they may need in order to make the most of your visit. In some cases, we will require a referral from your primary care physician. We would be happy to discuss this with you to ensure we have all we need to expedite the scheduling process. Please contact us by phone or email to begin the process.
Phone: NW Clinic for Voice & Swallowing 503-494-5947
Email: Otolaryngology -ENT Clinic
If you have a question for one of our providers, please email us.