MR Female Pelvis WWO for Brachytherapy Planning BODY Protocol
Scan Notes
Last updated: 5/11/2022
Charge as Pelvis WWO
Scanner preference: MR2
Coil: Torso Coil
This study is for radiation planning for endometrial, cervical and vaginal cancer.
- Scan time = Approximately 90 minutes
- NPO for 4 hours prior
- Void prior to exam start
Vaginal Gel Instructions:
- The clinician will indicate if vaginal gel or syed device is needed.
- Patient or brachytherapy physician will be placing intra-vaginal ultrasound gel while on MR table, using 60 cc slip-tip syringe.
- Instruct patient to place syringe tip deep, close to cervix.
- Patient or brachytherapy physician will fill vagina with gel while slowly removing syringe.
- The goal is to completely fill the vaginal vault near cervix with gel containing as little air as possible.
Post Processing:
- Reformats of 3D T2 at 1 mm to coronal and sagittal planes
- Generate ADC maps
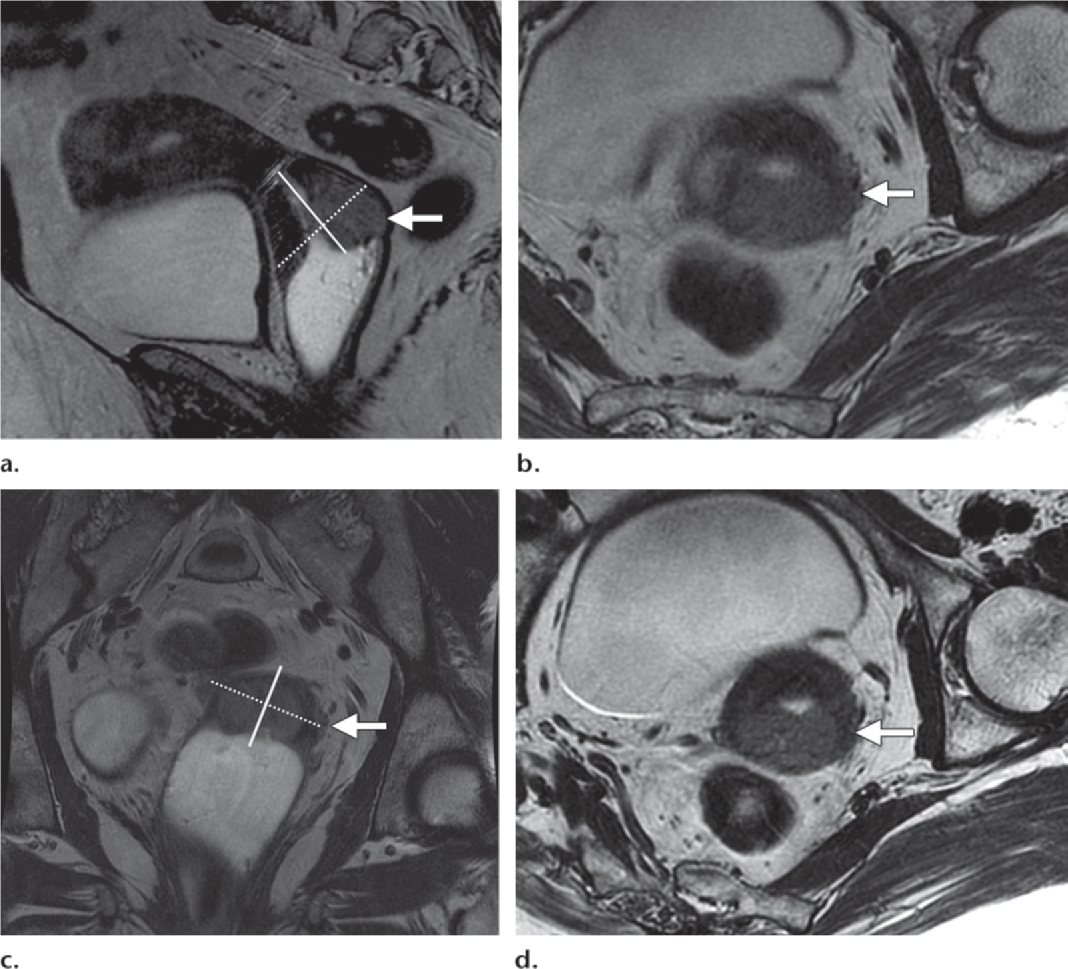
Figure 14. Value of double oblique high-resolution T2-weighted FRFSE MR images for depicting parametrial invasion.
(a) Sag T2: mass in the posterior cervical lip (arrow) and the acquisition plane (dashed line) of oblique axial images, which were obtained perpendicular to the long axis of the cervix (solid line).
(b) Ax oblique T2: obtained on the basis of Sag T2 shows the mass in the posterior cervical lip with possible tumor infiltration into the left parametrium (arrow).
(c) Cor T2; cervix, which angles to the left of the midline (arrow), and the angle of acquisition (dashed line) of the double oblique axial image perpendicular to the long axis of the laterally deviated cervix (solid line).
(d) Double oblique T2: along the axis of the cervix on the basis of the sagittal and coronal images shows an intact cervical stroma (arrow) between the tumor and the parametrium, excluding parametrial invasion at left. Double oblique images are valuable in eliminating the effects of volume averaging.
| ScanningPlane | Reminders | S/G (mm) | Fat Sat | Slice Position | Coverage | Comments |
|---|---|---|---|---|---|---|
| SAG T2 SSTSE | 4 / 0 | No | Confirm good coil placement | 350 mm. Sacrum to anterior abdominal wall. L4 to buttocks. | ||
| AX T2 3D TSE | Generate COR and SAG MPRs | 2 mm slice interpolated to 1 mm. Do not reduce slices; SNR is dependent on 3D volume. | No | Cover entire Vagina, Cervix, or Uterus depending on area of interest | 270 mm/ Fit to Patient. | Anterior sat band. |
| Oblique AX T2 TSE - Hig Res | Call rad for planning | 3 / 0 | No | Obtain true axial to organ of interest. Resulting image should be a true "doughnut" of organ. | 200-240 mm/ Fit to Patient. Matrix 512 x 256-512. Entire Vagina, Cervix, or Uterus depending on area of interest | Reminder: obliques, especially for cervical cancer, are planned off of TWO PLANES. |
| Oblique COR T2 TSE - High Res | Call rad for planning | 3 / 0 | No | Obtain true coronal to organ of interest. L-R phase direction | 200-240 mm/Fit to Patient. Minimize coverage to relevant anatomy | Reminder: obliques, especially for cervical cancer, are planned off of TWO PLANES. |
| Oblique SAG T2 TSE - High Res | Call rad for planning | 3 / 0 | No | Obtain true sagittal to organ of interest. Anterior Sat band to minimize wall motion. Phase A-P. | 200-240 mm/ Fit to Patient. Matrix 512 x 256-512. Minimize to relevant anatomy | Reminder: obliques, especially for cervical cancer, are planned off of TWO PLANES. |
| AX T1 3D THRIVE - High Res Pre | YES | High Resolution | 200-240mm/Fit to Patient | |||
| Hand-inject-contrast | ||||||
| AX T1 3D THRIVE - High Res Post | YES | Same as Pre | 200-240mm/Fit to Patient | |||
| SAG T1 3D THRIVE - High Res Post | YES | |||||
| COR T1 3D THRIVE - High Res Post | YES | |||||
| AX DWI Oblique | Free-breathing sequence, so please position slices accordingly. | 5 / 0 | SPIR | Match AX OBLIQUE | Match AX OBLIQUE | Trigger & track. B=0, 500, 1000. |